|
|
Abstract
Objective: Quercetin is a bioflavonoid noted for its
antihistamine release and antiproliferative effects. These
properties could theoretically prove beneficial in reversing the
inflammatory and proliferative responses in hypertrophic scars. The
aim of this study was to evaluate both preventive and curative
effect of quercetin on animal model of hypertrophic scars.
Materials and Methods: Full thickness four circular excisional wounds
were performed on each ear of ten rabbits. Quercetin cream was applied
immediately on one wound for four weeks as a preventive treatment and for eight
weeks on one hypertrophic scar as a curative treatment. Placebo cream was used
for the other two wounds.
Results: Clinically, after four weeks, hypertrophic scars were
developed in all non-treated and placebo-treated wounds. On the other hand, only
40% of quercetin-treated wounds healed with hypertrophic scars. The level of
histamine and hydroxyproline was significantly increased in placebo-treated
wounds in the preventive group. However, their levels in quercetin-treated
wounds were significantly decreased. In the curative group, after eight weeks
treatment with quercetin, only 20% of hypertrophic scars were flattened. While
histamine level was significantly decreased in quercetin-treated scars,
hydroxyproline level was insignificantly decreased as compared to
placebo-treated scars.
Conclusion: Due to its antihistamine effect beside its antifibrotic
effect, quercetin could be an effective preventive and to lesser extent an
adjuvant curative treatment for hypertrophic scars.
Introduction
Excessive dermal scarring in the form of hypertrophic scars and keloids continues to be a clinical problem[1].
Moreover, the functional and aesthetic
deformities associated with them remain a significant concern.[2, 3].
Because little is known about the pathophysiology of hypertrophic scarring,
an animal model is of great importance as a mean for studying the evolution of a
hypertrophic scar from early healing and for evaluating therapeutic modalities[1].
There is growing evidence that mast cells play a
fundamental role in tissue homeostasis, remodeling and repair. Mast cells store
and release various potent mediators, in particular histamine, proteases, lipid
mediators and cytokines through which they can influence different stages of
cutaneous wound healing.[4].
Wounding results in adaptive changes in
histidine decarboxylase enzyme activity and increases histamine forming
capacity.[5]. Increased histamine synthesis was reported in many tissues undergoing rapid
growth or repair.[6] Hydroxyproline is an amino acid formed from
proline incorporated into collagen and it is a subproduct of collagen
synthesis. Tissue hydroxyproline assay presents a parallel increase with tissue
collagen level and it is the best indicator of collagen synthesis and wound
healing.[7].
Quercetin, a bioflavonoid noted for its antiproliferative effects on both normal
and malignant cells and its antihistamine release effects. These properties
could theoretically prove beneficial in reversing the proliferative and
inflammatory responses in hypertrophic scars [8]
The aim of this study was to assess both preventive and curative effect of
quercetin on animal model of hypertrophic scars.
Materials and methods
The study was carried out on ten age-matched healthy white
male rabbits, weighing approximately 2 Kg each. Animals were housed under the
same controlled environmental conditions at the animal house of the pharmacology
department, Alexandria faculty of medicine, fed normal laboratory diet and they
had free access to tap water.
Animals were anesthetized with thiopental sodium (2.5mg/kg
I.V.). Full thickness four circular excisional wounds were performed down to
bare cartilage on the ventral surface of each ear by using a 4-mm punch biopsy.
A magnifying binocular loupe C 2.3x340mm (Heine, USA) was used. Hemostasis was
then obtained by applying pressure. All wounds were covered using an occlusive
polyurethane dressing (Tegaderm 3M, Minneapolis, Minn.) until the entire wound
appeared re-epithelialized on gross examination.
Photographs were obtained and treatment of one of four
wounds per ear was begun immediately with quercetin cream three times daily for
four weeks. The second wound was treated with placebo cream at the same time to
serve as control for the preventive group (n=10). The remaining two wounds per
ear remained untreated during this period till a hypertrophic scar was
established. After four weeks, treatment of the third wound that developed
elevated scar was begun three times per day for eight more weeks. The fourth
wound was treated with placebo cream to serve as control group for the curative
group (n=10).
The ingredients in the cream were modified from the formula
according to Katsarou et al.[9] Each 100 gm cream contain:
quercetin (Carl Roth, GmbH co. 76185 Karlsruhe, Germany) 7.5 gm, white soft
paraffin 9.5 gm, liquid paraffin 4.75 gm, acetyl alcohol 3.5 gm, glyceryl
monostearate 2.5 gm, cremophor RH40 4.00gm, methyl paraben 0.25gm, propyl
paraben 0.10gm, propylene glycol 10.00gm and water to 100gm. The placebo control
was identical in composition except for quercetin.
With the animals under anesthesia, serial photographs were taken. The scars on
the left ear were carefully excised and stored at -80°C for use in the
biochemical measurements of: 1-Hydroxyproline concentration which is considered
a reflection of collagen content as it comprises approximately ten percent of
collagen.[10] 2-Histamine concentration was carried out according to the method
of Shore et al.(11)
Statistical analysis[12]: All data were expressed as mean
+ standard deviation (SD). One-way analysis of variance (ANOVA) techniques were
used to examine the studied parameters. For pairwise comparisons among groups,
the least significance difference test (LSD) was used. P value was calculated
and statistical significance was set at (P<0.05)
Results
Clinically, after four weeks, hypertrophic scars were developed in all
non-treated and placebo-treated wounds. On the other hand, only 40% of quercetin
treated wounds healed with hypertrophic scars. In the curative group, after
eight weeks treatment with quercetin, 20% of hypertrophic scars were flattened.
At the same time, simultaneous reduction in the prominence of the
placebo-treated scars occurred in 10% of the scars. (Figure 1).
The concentration of hydroxyproline in placebo-treated scars was
significantly high at four weeks as compared to unwounded skin (7.92 + 0.27 vs
3.44+0.14mg/mg tissue P<0.001). The quercetin-treated wounds had significantly
decreased hydroxyproline level than placebo-treated wounds at four weeks
(preventive group) (4.80 + 0.28 vs 7.92 + 0.27
mg/mg tissue P<0.001). In the
curative group, the concentration of hydroxyproline decreased in quercetin-treated
scars. Nevertheless, there was no significant difference in the scars treated by
quercetin compared to those treated by placebo (9.91 + 0.28 vs 10.15 + 0.36 mg/mg tissue P >0.05). (Table 1)
At four weeks, compared to unwounded skin, the placebo-treated scars in the
preventive group contained triple the level of histamine (6.39 + 0.9 vs 2.11+
0.17mg/g tissue P<0.001). Moreover,
histamine continued to increase after eight more weeks (14.01 + 1.22
mg/g tissue). However, it was significantly
less in quercetin-treated scars than placebo-treated scars in both preventive
group (4.49 + 0.52 vs 6.39 + 0.9
m/g tissue
P<0.001) and curative group (5.37 + 0.49 vs 14.01 + 1.22
mg/g tissue P<0.001). (Table 1)
 |

|

|
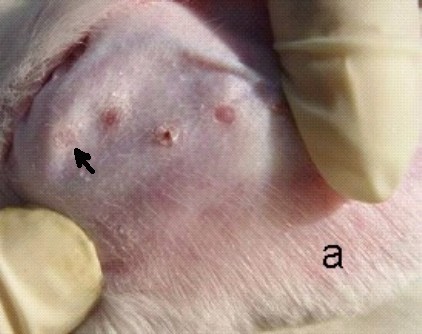
| Figure 1: a-Two weeks photo showing healing
with flat scar only in quercetin treated wound (preventive group); b- Four
weeks photo showing flat scar in quercetin treated wound and hypertrophic
scar in the rest (preventive group); c- Twelve weeks photo showing
flattening of the hypertrophic quercetin treated scar and the control scar
(encircled) is still hypertrophic (curative group) |
Table1: Effect of quercetin on hydroxyproline and histamine concentration in rabbit’s ear wounded skin (mean
+ SD).
| |
Unwounded skin (n=10) |
Preventive
group (n=10) |
Curative group (no=10) |
|
Quercetin treated |
Placebo
treated |
Quercetin
treated |
Placebo
treated |
| Hydroxyproline (mg/mg
tissue) |
3.44+0.14 |
4.80 + 0.28*# |
7.92 +0.27# |
9.91 + 0.28# |
10.15 + 0.36# |
| Histamine (m/mg
tissue) |
2.11+ 0.17 |
4.49 + 0.52*# |
6.39 + 0.9# |
5.37 +0.49*# |
14.01 + 1.22# |
| * Significant as compared to placebo-treated
group. # Significant as compared to unwounded skin.
|
Discussion
Hypertrophic scars are abnormal healing responses that
develop as a result of an exaggerated proliferation of dermal fibroblasts after
skin injury and are characterized by excess accumulation of collagen in the
wound.[13]. The development of this abnormal pattern of healing
has been associated with an extended period between wounding and
re-epithelialization of the wound, resulting in a prolonged inflammatory phase.
This may occur as a result of complications such as an infection, a foreign body
within the wound, excessive tension on the wound or persistent mobilization of
the wound edges[14]. However, in some cases, the pathogenesis
of hypertrophic scarring is unknown.[8].
Hypertrophic scars generally appear within four weeks
after trauma, enlarge for three to six months, remain static for several months
and gradually regress in terms of erythema, size, and irritability over
approximately one year[2, 15]. A peak in collagen synthesis at six months is
followed by a decrease in synthesis and parallels the clinical changes[16]. In
the present work, similar to Saulis[8] group, clinically at
four weeks hypertrophic scars were developed in all non-treated and placebo
treated wounds. Morris et al[1] ,in the early model of scarring
in rabbits, found that these scars tended to decrease in prominence subsequent
to day 22, although it has previously been observed in the laboratory that some
remain elevated for months. Reduction in the prominence of scars in this study
occurred in 10% of placebo treated scars at twelve weeks.
During the present study, there was a continuous increase in the amount of
collagen measured as hydroxyproline. This result supports the conclusion that
the process of scar remodeling including collagen cross linking and active
collagen turnover occurs from one month and continues to one year [17].
Moreover, fibrotic conditions such as keloids and hypertrophic scars have excess
connective tissue with the collagen being the major contributor[18]. Mast cells
are identified in both of these fibrotic conditions and are implicated as a
possible contributor to their development and possibly involved in the collagen
scar-like organization. They specifically influence granulation tissue
organization during wound repair[4, 19]. Rothe et al[20]
reported that products of mast cell degranulation (in vitro) are conspicuously
implicated in these pivotal events. One such mast cell product, histamine,
significantly increased fibroblast proliferation and collagen synthesis[4, 20, 21].
Reich et al[22] observed that immediately after incisional
wounding in a domestic pig model, mast cell numbers increased rapidly and
subsequently peaked two days after wounding, declined at a relatively constant
rate from day two to four and then returned gradually to normal levels at day
fourteen. This fluctuation of mast cell numbers and histamine release correlates
well with the concomitant formation of granulation tissue, the hallmark of early
wound healing[23]. This decline in mast cell number is in contrast to the
cellular events seen in hypertrophic scars, in which increased numbers of mast
cells persist indefinitely with an associated elevation of tissue histamine[24].
These fibrotic lesions reportedly exhibit as much as 10 to 100 times more mast
cells than normal human skin[25]. The results of the present work showed that,
after four weeks, the level of histamine in placebo treated wounds was triple
the normal level in the preventive group. Moreover, it continued to increase
after eight more weeks.
Although many articles have been published on the management of hypertrophic
scars and keloids, there is no universally accepted treatment protocol.
Prevention of them remains the best strategy[17]. Quercetin is
a bioflavonoid known to inhibit free radical processes in cells[9]. It is able
to protect cutaneous tissue-type cell populations, fibroblasts/keratinocytes and
endothelial cells of human origin from cytotoxic oxidative stress induced by
protracted depletion of cellular glutathione[26]. In addition, quercetin has
been shown to have an anti-inflammatory effect by stabilizing mast cell
membranes and inhibit histamine release from basophils and mast cells as well as
an antiproliferative effect in both normal and malignant cells of various
types[8, 27]. It causes cell cycle arrest and
apoptosis[28, 29].
Limiting inflammation is paramount in the control of scar growth and
scar-associated symptoms[30]. The anti-inflammatory effect of
quercetin, that was previously reported [31], may be a reasonable explanation of
its antifibrotic effect. In the current study, hypertrophic scars developed in
less than half of quercetin treated wounds. Inhibition of excess collagen
formation could be a consequence of early control of histamine release as a
significant decrease in the level of histamine and hydroxyproline was proved in
the preventive group of this study. The decrease in histamine, as suggested by
Lee et al[32], was due to inhibition of mast cell degranulation. The antioxidant
effect of quercetin might be another explanation for its antifibrotic action.
Free radicals are likely to contribute to progressive fibrosis and excessive
scar formation in abnormal wound healing[33]. These substances, although
important for eliminating infection, can damage surrounding tissue and host
cells and initiate further inflammation and pro-inflammatory mediator
production. The importance of reactive oxygen species (ROS) in the development
of fibrosis is supported by the fact that antioxidants have been shown to be
antifibrogenic.[9, 33]. However, the role of ROS in cutaneous scarring remains
under investigation. Another possible mechanism for the antifibrotic action of
quercetin is its apoptotic effect. It inhibits insulin-like growth factor I, a
potent mitogen and inhibitor of apoptosis for cell types[29]. IGF-I
has been shown to stimulate fibroblast proliferation and enhances collagen
synthesis[34].
In another study [8], a significant improvement in dermal
collagen organization was noted on comparing mederma-treated with untreated
scars on rabbit’s ear hypertrophic scar. However, there was no decrease in scar
height. They suggested two possibilities, either the conversion of immature to
mature collagen is accelerated in some fashion with no net decrease in overall
collagen production by fibroblasts or the treatment period of four weeks was too
brief to detect a significant decrease in scar hypertrophy. Although the
treatment period was extended to eight weeks in the present study with
significant reduction in histamine level, flattening occurred only in 20% of
hypertrophic scars with insignificant decrease in hydroxyproline level. It seems
that early control of inflammatory stage by starting treatment concomitantly
with skin incision may decrease or block histamine release and its subsequent
stimulation of fibroblast proliferation and excessive collagen synthesis.
However, it may not affect collagen breakdown and degradation in mature
hypertrophic scars. Furthermore, quercetin concentration may have a role. Lim et
al [35] found that treatment of fibroblasts derived with
quercetin in a dose-dependant manner led to a significant inhibition of
fibroblast proliferation.
In conclusion, due to its anti-histamine effect beside its antifibrotic effect,
quercetin could be an effective preventive and to lesser extent adjuvant
curative treatment for hypertrophic scars.
Acknowledgment:
The authors would like to thank Professor Osama Abdala, professor of
pharmaceutics, Alexandria faculty of pharmacy for his assistance in preparing
the quercetin cream.
References
1. Morris D, Wu L, Zhao L, Bolton L, Roth S, Ladin D, Mustoe T. Acute and chronic animal models for excessive dermal scarring: Quantitative studies. Plast Reconstr Surg 1997; 100:674-81.
2. Niessen F, Spauwen P, Schalkwijk J, Kon M. On the nature of hypertrophic scars and keloids: A review. Plast Reconstr Surg 1999; 104:1435-58. (Med Line)
3. Uppal R, Khan U, Kakar S, Talas G, McGrouther A. The effects of a single dose of 5-fluorouracil on keloid scars: A clinical trial of timed wound irrigation after extralesional excision. Plas Reconst Surg 2001; 108:1218-24.
4. Artuc M, Steckelings M, Henz B. Mast cell-fibroblast interactions: Human mast cells as source and inducers of fibroblast and epithelial growth factors. J Invest Dermatol 2002; 118:391-5.
5. Fitzpatrick D, Fisher H. Histamine synthesis, imidazole dipeptides and wound healing. Surgery 1982; 91:430-4.-8.
6. Singer A, Clark R. Cutaneous wound healing. N Engl J Med 1999; 341:738-46.
7. Kahlson G, Nilsson K, Rosengren E, Zenderfeldt B. Wound healing as dependent on the rate of histamine formation. Lancet 1960; 2: 230-4.
8. Saulis, Alexandrina S, Mogford, Jon H, Mustoe, Thomas A. Effect of Mederma on hypertrophic scarring in the rabbit ear model. Plast Reconstr Surg 2002; 110:177-83.
9. Katsarou A, Davoy E, Xenos K, Armenaka M, Theoharides T. Effect of an antioxidant (quercetin) on sodiumlauryl-sulfate-induced skin irritation. Contact Dermatitis 2000; 42:85–9.
10. Cheng P. An improved method for the determination of hydroxyproline in rat skin. J Invest Dermatol 1969; 53:112-5.
11. Shore P, Burkhalter A, Cohn V. A method for fluorometric assay of histamine in tissues. J Pharmcol Exp Ther 1959; 127:182-6.
12. Hill B. Principles of medical statistics, 9th ed. London. Lancet limited publication 1971, 147; 383-6.
13. Saray Y, Güleç A. Treatment of keloids and hypertrophic scars with dermojet injections of bleomycin. J European Acad Dermatol Venereol 2003; 17:150-1.
14. Clark R. Basics of cutaneous wound repair. J Dermatol Surg Oncol 1993; 19:693-706.
15. Muir I. On the nature of keloid and hypertrophic scars. Br J Plast Surg 1990; 43: 61-9.
16. Sahl W, Clever H. Cutaneous scars: Part I. Int J Dermatol 1994; 33:681-91.
17. Alster T, Tanzi E. Hypertrophic scars and keloids: etiology and management. Am J Clin Dermatol 2003; 4: 235-43.
18. Rahban S, Garner W. Fibroproliferative scars. Clin Plast Surg 2003; 30:77-89.
19. Moyer K, Saggers G, Ehrlich P. Mast cells promote fibroblast populated collagen lattice contraction through gap junction intercellular communication. Wound Repair Regen 2004; 12:269-75.
20. Rothe M, Nowalk M, Kerdel F. The mast cell in health and disease: A greater role. J Am Acad Dermatol 1990; 23:615-24.
21. Garbuzenko E, Nagler A, Pickholtz D, Gillery P, Reich R, Maquart F, Levi-Schaffer F. Human mast cells stimulate fibroblast proliferation, collagen synthesis and lattice contraction: A direct role for mast cells in skin fibrosis. Clin Exp Allergy 2002; 32:237-46.
22. Reich J, Cazzaniga A, Mertz P, Kerdel F, Eaglstein W. The effect of electrical stimulation on the number of mast cells in healing wounds. J Am Acad Dermatol 1991; 25:40-6.
23. Sasaki A, Mueller R, Xi G, Sipe R, Buck D, Hollinger J. Mast cells: An unexpected finding in the modulation of cutaneous wound repair by charged beads. Plast Reconstr Surg 2003; 14: 1446-53.
24. Hermes B, Feldmann-B?ddeker I, Welker P, Algermissen B, Steckelings M, Grabbe J, Henz B. Altered expression of mast cell chymase and tryptase and of c-kit in human cutaneous scar tissue. J Invest Dermatol 2000; 114:51-5.
25. Tharp M. The mast cell and its role in human cutaneous diseases. Prog Dermatol 1987; 21:1-5.
26. Skaper S, Fabris M, Ferrari V, Carbonare M, Leon A. Quercetin protects cutaneous tissue-associated cell types including sensory neurons from oxidative stress induced by glutathione depletion: Cooperative effects of ascorbic acid. Free Radical Biol Med 1997; 22:669-78.
27. Alexandrakis M, Singh L, Boucher W, Letourneau R, Theofilopoulos P, Theoharides T C. Differential effect of flavonoids on inhibition of secretion and accumulation of secretory granules in rat basophilic leukemia cells. Int J Immunopharmacol 1999; 21:379-90.
28. Yoshida M, Yamamoto M, Nikaido T. Quercetin arrests human leukemic T-cells in late G1 phase of the cell cycle. Cancer Res 1992; 52:6676–81.
29. Wei Y, Zhao X, Kariya Y. Induction of apoptosis by quercetin: involvement of heat shock protein. Cancer Res 1994; 54:4952–7.
30. Danielson J, Walter R. Salicylic acid may be useful in limiting scar formation. Plast Reconstr Surg 2004; 114:1359-61.
31. Taguchi K, Hagiwara Y, Kajiyama K, Suzuki Y. Pharmacological studies of Houttuyniae herba: The anti-inflammatory effect of quercetin. Yakugaku Zasshi 1993; 113:327-33.
32. Lee E, Choi E, Cheong H, Kim Y, Ryu S, Kim K. Anti-allergic actions of the leaves of Castanea crenata and isolation of an active component responsible for the inhibition of mast cell degranulation. Arch Pharm Res 1999; 22: 320-3.
33. Phan T, Sun L, Bay B, Chan S, Lee S. Dietary compounds inhibit proliferation and contraction of keloid and hypertrophic scar-derived fibroblasts in vitro: Therapeutic implication for excessive scarring. J trauma 2003; 54: 1212-24.
34. Phan T, See P, Tran E, Nguyen T, Chan S, Lee S. Suppression of keloid derived fibroblasts by quercetin: its therapeutic potential use in the pathway and collagen insulin-like growth factor signaling expression in treatment and /or prevention of keloids. Br J Dermatol 2003; 148:544–52.
35. Lim I, Phan T, Lee S, Huynh T, Longaker M. Quercetin inhibits keloid and hypertrophic scar fibroblast proliferation and collagen production. ANZ J Surg 2003; 73:286.
© 2005 Egyptian Dermatology Online Journal
|