|
|
Abstract
Osteogenesis imperfecta (OI) type I is a dominantly inherited, generalized connective tissue disorder characterized mainly by bone fragility and blue sclerae. We report on two male patients, aged 56 and 58 years, who presented with a combination of OI with psoriasis vulgaris.
The mutations could be localized within the COL1A1-gene: in case 1 a heterozygous deletion of cytosine base in position 3494 of exon 48 (c.3494del), in case 2 a heterozygous point mutation in exon 50 (c.3975G>A).
Clinically blue sclerae, bone fragility, history of multiple bone fractures, deformities of long bones, and osteoporosis were evident in both patients. Both suffered from hearing impairment. Their psoriasis was of the chronic plaque type. To the best of our knowledge these are first case reports about the combination of both disorders.
Introduction
Osteogenesis imperfecta (OI) type I is a dominantly inherited, generalized connective tissue disorder characterized mainly by bone fragility, hearing loss and blue sclerae. Additional features of OI include hearing loss of conductive or mixed type in about 50% of families, tinnitus, and vertigo.[3] Furthermore thin, easily bruised skin, moderate joint hypermobility and kyphoscoliosis, hernias, and arcus senilis are quite common.[1],[2]
Individuals with OI type I have distinctly blue sclerae which remain intensely blue throughout life, in contrast to the sclerae in OI type III and OI type IV which may also be blue at birth and during infancy. The intensity of the blue fades with time such that these individuals may have sclerae of normal hue by adolescence and adult life.[3]
OI type I phenotype can be produced by mutation in either the COL1A1 gene (120150) or the COL1A2 gene (120160) and possibly in other genes. In most cases, 'functional null' alleles of COL1A1 on chromosome 17 or COL1A2 on chromosome 7 lead to reduced amounts of normal collagen I.[1] Hartikka et al.[1] found that patients with COL1A1 mutations more frequently had blue sclerae than those with COL1A2 mutations. In addition, patients with COL1A2 mutations tended to be shorter than those with COL1A1 mutations.
A coincidence of OI with skin disease is uncommon. The only exception to this rule might be elastosis perforans serpinginosa, a disease more often seen in inherited connective tissue disease.[4]
Case reports
The two cases were male patients who were referred to our department because of recalcitrant plaque-type psoriasis vulgaris (Figs. 1 and 2).
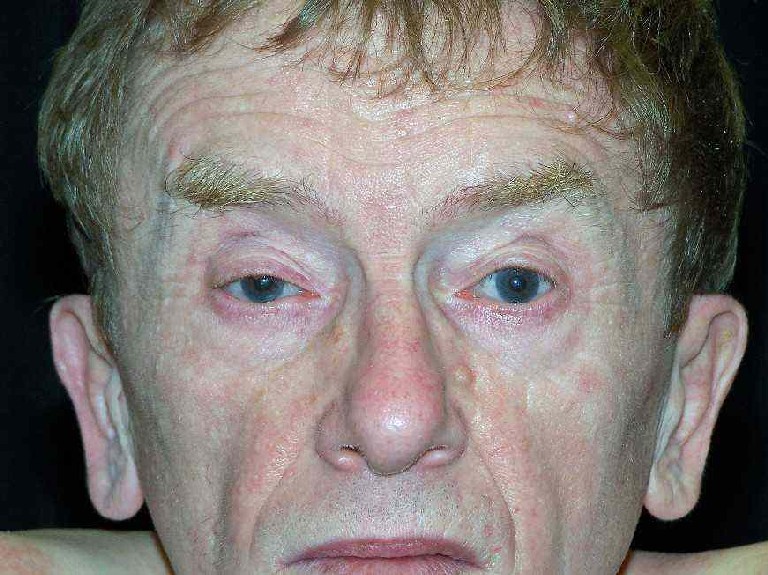
Figure 1: Case 1
A) Blue sclerae.
B) and C) Psoriatic plaques on the thorax and slight
thoracic deformity due to scoliosis (B
– front; C – back). |
Figure 2: Case 2
A) Blue sclerae.
B) and C) Psoriatic plaques on the hips and the back,
thoracic deformity and kyphoscoliosis (B – front; C – back). |
In both the combination of blue sclerae, a history of multiple bone fractures and bone deformities suggested a possible affection by OI.Clinical investigations, computerized tomography, and genetic analysis confirmed the diagnosis of OI type I. In case two there was a family history for OI but not in case 1. Details are summarized in table 1.
| |
Case 1 |
Case 2 |
|
Age/ sex |
56/ male |
58/ male |
|
Height/ body weight
|
165 cm/ 65 kg |
165 cm/ 43 kg |
|
Familiy history |
positive for psoriasis |
positive for OI |
|
Bone fragility and fractures |
+ |
+ |
|
Bone mineral density (BMD) |
55-60% of normal BMD |
78-80% of normal BMD
T score -3.1 to -3.4 |
|
Bone deformities |
coxa vara, femura vara et antecurvata, left convex
scoliosis |
coxa vara, kyphoscoliosis |
|
Bone histology |
not done |
low-turnover osteoporosis |
|
Arthrosis |
coxarthrosis, gonarthrosis |
coxarthrosis, gonarthrosis, sponylosis deformans |
|
Hearing |
bilateral high tune
hearing impairment |
bilateral high tune
hearing impairment |
|
Eyes |
blue sclerae |
blue sclerae |
|
Laboratory investigations |
erythrocytes 4.48 Tpt/L
(normal range 4.6-6.2),
Hb 8.2 mmol/L (8.6-12.1),
haematokrit 0.39 L/L
(0.40-0.54) |
IgE 3140 U/L (0-100) |
|
Genetics |
c.3494del in exon 48 of COL1A1- gene leading to
a stop codon,
heterozygous |
c.3975G>A point mutation in exon 50 of the
COL1A1-gene leading to a stop codon (p.Trp1325X),
heterozygous |
|
Associated diseases |
psoriasis vulgaris |
psoriasis vulgaris, chronic obstructive bronchitis
|
Table 1:
Summary of the two cases with co-morbidity of psoriasis vulgaris and osteogenesis imperfecta (OI) type I
In both cases psoriasis was observed from the youth where it was possibly triggered by streptococcal infection in the early beginning. They presented with chronic plaque-type erythemato-squamous plaques, nail involvement and affection of the capillitium.
There was no clinical evidence or medical history suggesting
psoriasis arthritis. They were treated by a combination of topical therapy and UVB-irradiation.
Discussion
We report on two male patients with a combination of OI type I and widespread psoriasis vulgaris. Psoriasis itself is characterized by a high turnover bone remodelling not restricted to patients with psoriatic arthritis.[5] In combination with steroid therapy or hormonal imbalance, however, this may lead to a diminished bone mineral density.[6],[7] In contrast, a low turnover bone remodelling was detected in case 2.
Bone histomorphometric studies in children affected by OI type I showed both reduction in trabecular number and trabecular thickness leading to decreased cancellous bone volume. Surface-based parameters of bone remodelling were increased in OI indicating increased recruitment of remodelling units. Wall thickness was decreased but no defect in matrix mineralization was found.[8]
The combination of OI and psoriasis seems to increase the risk of adverse effects of systemic steroid therapy on bone mineral density. Intraarticular and systemic steroids are commonly in use for psoriatic arthritis. They may reduce bone mineral density in contrast to methotrexate.[9] A case of fully reversible tubular toxicity with consecutive metabolic osteopathy following systemic fumaric acid therapy was reported in a 46-year-old woman with psoriasis and DeToni-Debre Fanconi syndrome.[10] This secondary effect of oral fumaric acid therapy obviously occurs very rarely and was a result of hypophosphataemic osteomalacia due to complex disturbances of the renal tubular system. Weather UV-therapy of psoriasis may have a beneficial effect on OI associated osteoporosis is questionable, since the major biochemical alterations are found in collagen production but not vitamin D metabolism.[1]
In summary, despite the rarity of OI, it should be also suspected and confirmed in psoriasis patients when the typical triade of symptoms is observed, i.e. bone fragility, hearing loss and blue sclerae.
References
1. Rauch F, Glorieux FH. Osteogenesis imperfecta. Lancet 2004; 363: 1377-1385.
2. Hartikka H, Kuurila K, Korkko J, et al. Lack of correlation between the type of COL1A1 or COL1A2 mutation and hearing loss in osteogenesis imperfecta patients. Hum Mutat 2004; 24: 147-154.
3. Sillence DO. Osteogenesis imperfecta nosology and genetics. Ann NY Acad Sci 1988; 543: 1-15.
4. Mehta RK, Burrows NP, Payne CM, et al. Elastosis perforans serpinginosa and associated disorders. Clin Exp Dermatol 2001; 26: 521-524.
5. Hein G, Abendroth K, Müller A, Wessel G. Studies on psoriatic osteoarthropathy. Clin Rheumatol 1991; 10: 13-17.
6. Cooper C, Poll V, McLaren M, et al. Alterations in appendicular skeletal mass in patients with rheumatoid psoriasis and osteoarthropathy. Ann Rheumat Dis 1988; 47: 481-484.
7. Del Puente A, Mantova D, Mandes MG, et al. Osteoporosi et artrite psoriasica. Rheumatismo 1994; 46: 70-73.
8. Rauch F, Travers R, Parfitt AM, Glorieux FH. Static and dynamic bone histomorphometry in children with osteogenesis imperfecta. Bone 2000; 26: 581-589.
9.
Cranney AB,
McKendry RJ,
Wells GA,
et al.
The effect of low dose methotrexate on bone density. J
Rheumatol 2001; 28: 2395-2399.
10.
Fliegner L, Spiegel P. Osteomalazie als offensichtlich
seltene Nebenwirkung der oralen Fumarsäuretherapie.
Sekundäres DeToni-Debre-Fanconi-Syndrom beim Erwachsenen.
Hautarzt 1992; 43: 554-560.
© 2006 Egyptian Dermatology
Online Journal
|