|
|
Abstract
Syringoma is a benign, eccrine sweat gland tumor. The typical clinical appearance of syringoma is firm, skin- colored to brown papules on the lower eye lids of middle - aged women. Familial syringoma is rare, but possibly is underestimated in prevalence. Eruptive syringoma, a separate entity, presents mostly in adolescents as clusters of numerous papules on the upper half of the body. Familial eruptive syringoma is a very rare clinical variant with only few reports in world literature. Case study
Three sisters and two brothers presented to our Dermatology & Venereology department with disfiguring skin lesions asking for
treatment. Their mean age was 27 years.
Case 1: A 23 year old female presented with asymptomatic lesions on abdomen, axillae, and neck
(fig1)
 | Fig 1:
Showing abdominal lesions in case 1 |
|
Case 2 and Case3: They are sisters of the first case (27, 36 year old respectively). They had similar distributed lesions on forearms, chest and axillae
(fig 2, 3).
 | Fig
2: Showing forearm lesions in case 2 |
|
 | Fig
3: Showing neck lesions in case 3 |
|
Case 4 and Case 5: They are brothers of the previous cases, of 22 and 32 year old respectively. The lesions were fewer than in female cases, on axillae, neck, chest and abdomen
(fig 4).
 Fig
4: Showing axillary lesions in case 4
All lesions appeared as clusters of numerous skin colored and
hyperpigmented rounded or flat-topped papules |
|
On examination of their father, similar lesions appeared on lower eye lids, cheeks and anterior surface of neck. There is a history of consanguinity. The lesions in all cases appeared as symmetrically distributed clusters of numerous skin colored and hyperpigmented rounded or flat-topped papules 1 to 3 mm in diameters. These lesions are asymptomatic first appeared at puberty, but additional lesions had developed later. Biopsies were taken from different skin lesions in all patients. Results of histopathologic examination of lesions revealed aggregations of small tubular structures, lined by two rows of epithelial cells. Most of which are characterized by comma- like tails giving them a tadpole shape. They are embedded in a fibrous connective tissue stroma in the dermis (fig 5). These histopathologic findings were consistent with syringoma.
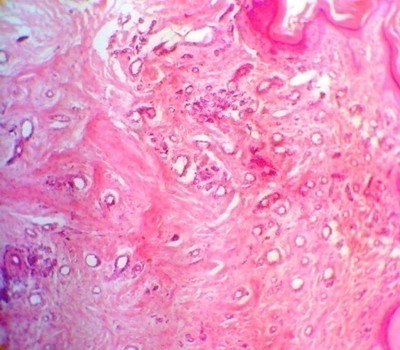 | Fig
5: Photomicrograph showing numerous, scattered, dermal, small
ducts lined by two rows of epithelial cells ; some of which have
epithelial cords with comma-like tails embedded in a sclerotic
stroma(H&E x150). |
|
Discussion
Syringoma is derived from Greek word syrnx, which means pipe or tube. It is a benign adnexal tumor of eccrine origin. It is seen commonly in females [1]. It is most common on the eye lids [2].Other clinical variants, eruptive [3], linear [2], familial [4], vulvar [5], penile [6], scalp [3], acral [7] and plaque-type syringomas [8] have been described. Eruptive syringoma is a clinical variant with many reports in world literature [3]. It is characterized by small, flesh-colored papules that occur in successive crops on the anterior body surface [9]. It arises in the peripubertal period. The lesions are bilateral, symmetrical, and have both follicular and non-follicular distribution [10]. In eruptive syringoma, a rare variant first described by Jacquet and Darier in 1987, the lesions occur in large numbers and in successive crops on the anterior chest, neck, upper abdomen, axillae, and periumbilical region at puberty or during childhood [6]. Eruptive syringomas are described more frequently in patients with Down's syndrome, and patients with Ehlers-Danlos syndrome [6]. In our cases no association have been detected. Some literature has challenged the notion that eruptive syringoma is neoplastic. These authors maintain that eruptive syringoma actually represents a hyperplastic response of the eccrine duct to an inflammatory reaction. The pruritus which is sometimes associated with syringomas is another argument in favor of this hypothesis, while in our cases pruritus is absent. This hypothesis makes it difficult, however, to explain the familial occurrence of syringoma. Most authors still believe syringoma to be of sporadic or hereditary etiology [10,11,12]. Reed [13] described a family in which 7 females and 1 male in 4 generations were affected. Familial syringoma is rare, but possibly is underestimated in prevalence. In most reported families, syringoma have been observed to occur in an autosomal dominant pattern [14]. While familial eruptive syringoma is seldom reported, one author reported a family (mother, daughter and son) with dominantly inheritance eruptive syringoma. On contrary to our cases, syringomas were not presented on eye lids of any one of this family [15]. To the best of our knowledge, familial eruptive syringoma is very rare with only few cases have been reported. In most reported families, syringomas have been observed to be more common in females. This female preponderance in both sporadic and familial forms of syringoma is well recognized but remains unexplained [4]. An association of syringoma with hormonal factors has been
suggested; in particular the size of vulval syringomas may increase during pregnancy [6]. The lesions of syringoma may be disfiguring and often pose significant cosmetic concerns for patients [16]. There is no satisfactory treatment for wide spread syringoma. Surgical or chemical destruction involve some risks of scarring. Many treatment modalities such as dermabrasion, electrodessication with curettage and scissors excision have been tried with some success in limited sites [17]. Because they are located in the dermis and often numerous, unfortunately, different modalities of therapy yield poor cosmetic results . There is no standard treatment for eruptive syringomas. Although carbon dioxide lasers, topical tretinoin and trichloroacetic acid have been found to be useful, none eliminates the possibility of recurrence. Syringoma may also undergo
spontaneous regression with age [3]. The patients presented here asked for treatment, but after discussion of known possibilities, they refrained from treatment References
1.
Horenstein MG. Syringoma. eMedicine 2007; 23.
2.
Kakinuma H and Urahashi J. Multiple axillary papules-Quiz case. Arch
Dermatol.2004; 140(9): 1161- 1168.
3.
Kumaran MS and Kanwar A. Multiple Syringomas of the forehead and scalp: An
unusual presentation. Indian J Dermatol 2005; 50(3): 171- 2.
4.
Gupta LK and Raman M. Familial Syringoma. Indian J Dermatol Venereol Leprol
1997; 63(6): 373- 5.
5.
Huang YH, Chuang YH, Kuo TT, Yang LC, and Hong HS. Vulvar Syringoma. J Am
Acad Dermatol 2003; 48(5): 735- 9.
6.
Hertyazdi M, Niedermeier A, Horster S, and Krause W. Penile Syringoma in a
14-year-old boy. Eur J Dermatol 2006; 16(3): 314- 5.
7.
Martin-Garcia RF and Munoz CM. Acral Syringomas presenting as a
photosensitive papular eruption. Cutis 2006; 77(1): 33- 6.
8.
Suwattee P, MC Clelland MC, Huiras EE, Warshaw EM, Lee PK, Kaye VN, MC
Calmont TH, Niehans GA. Plaque-type Syringoma. J Cutan Pathol 2008; 35(6):
570-4.
9.
Garrido-Ruiz MC, Enguita AB, Navas R, Polo I, and Rodriguez Peralto JL.
Eruptive Syringoma Developed Over a Waxing Skin Area. Extraordinary Case
Report. Am J Dermatopathol 2008; 30(4): 377- 380
10.
Hsiung SH. Eruptive Syringoma. Dermatol on line J 2005; 9(1): 14.
11.
Guitart J, Rosenbaum MM, Requena L. Eruptive syringoma a misnomer for a
reactive eccrine gland ductal proliferation? J Cutan Pathol 2003; 30: 202-
5.
12.
Corredor F, Colen PR, Tschen JA. Syringomatous changes of eccrine sweat
ducts associated with prurigo nodularis. Am J Dermatopathol 1998; 20(3):
296- 301.
13.
Reed WB.Genetische Aspekte in der Dermatologie.Hautar zt 1970; 21: 8- 16.
14.
Draznin M. Hereditary syringomas: A case report. Dematol on line J 2004;
10(2): 19.
15.
Patrone P, PatrizI A. Familial Eruptive Syringoma.G Ital Dermatol Venereol
1988; 123(7-8): 363- 5.
16.
Frazier CC, Camacho AP, and Cockerell CJ. The treatment of eruptive
syringomas in an African American patient with a combination of
trichloroacetic acid and Co2 laser destruction. Dermatol Surg 2001; 27(5):
489- 92.
17.
Teixeira M, Ferreira M, Machado S, Alves R, and Selores M. Eruptive
Syringomas. Dermatol on line J 2005; 11(3): 34.© 2009 Egyptian Dermatology Online Journal |
