|
|
Abstract:
Background and
Objectives:
Acne Keloidalis nuchae (AKN)
is a chronic inflammatory process involving the hair follicles of the nape
of the neck. It initially manifests as mildly pruritic follicular-based
papules and pustules. As folliculitis persists, keloidal plaques eventuate.
This study was performed
to evaluate the therapeutic effect of long pulsed ND: YAG laser in treatment
of different lesions of AKN.
Patients and methods:
Twenty-five male patients
were complaining of AKN. Inflammatory papules and keloidal plaques were
treated using long pulsed ND: YAG 1064 nm. Sessions were
performed at monthly basis for 6 sessions. Evaluation included papule count,
keloidal plaque size and pliability assessment before, every two sessions
and at the end of treatment. Patient self- assessment included evaluation of
pain, pruritus and cosmetic appearance at the end of treatment. Follow up
was carried out for 3 months.
Results:
A 31% reduction in the
mean papular lesions count were observed as early as the 2nd
laser sessions with, 68.2% reduction after the 4th laser session
and 90.9 % reduction at the end of treatment p<0.0001. Significant
reduction in the mean area of keloidal plaque size was initially seen after
the 4th laser session and 70.4% reduction was obtained at end of
laser sessions. Significant keloidal plaques softening versus baseline was
demonstrated after the 4th laser session (p<0.0001). Improvement
of subjective symptoms was elicited. The only side effect was temporary hair
loss in five patients where lesions occurred above the hairline.
Conclusion:
Long pulsed ND: YAG laser
(1064nm) is an effective treatment of both papules and keloidal lesions of
AKN where significant reduction in papule count, size, softening of keloidal
plaques obtained with no recurrence in the three months follow up period.
Introduction:
Acne keloidalis nuchae (AKN),
also known as folliculitis keloidalis, is a chronic inflammatory process
involving the hair follicles in the occipital region of the scalp and
posterior aspect of the neck. It is characterized by the presence of
follicular papules and pustules which enlarge forming confluent thickened
keloid- like plaques [1].
The condition occurs mainly in post pubescent males between the ages of 14
and 25 years, however, a few female patients have also been reported [2,3].
AKN occurs most frequently in individuals of African descent [2].
The cause of AKN remains unclear; however, penetration of cut curved hairs
into the skin in genetically predisposed individuals is the most accepted
theory [4].
The notion that AKN lesions are caused by ingrowing hair is analogous to the
situation in pseudo- folliculitis barbae [4,5].
Although various treatment modalities have been used in the management of
AKN such as topical and intralesional steroids, antibiotics, retinoids,
surgical excision with primary closure and excision with grafting, the
disease is often refractory with reported recurrence [6].
Laser technology such as CO2 and long pulsed diode laser has been
used in treatment of AKN [7,8].
Based on the postulation that the pathogenesis of AKN is similar to pseudo-
folliculitis barbae, long pulsed diode laser 810 nm has been used to treat
papular and nodular lesions of AKN [8].
Long pulsed ND: YAG laser 1064nm has been proven to be a safe and effective
option for treatment of pseudo- folliculitis barbae in dark skinned patients
with no pigmentary changes [9].
This study was designed to evaluate the efficacy of long pulsed ND: YAG
laser in treatment of different lesions of AKN; papular and keloidal
plaques.
Patients and methods:
Study design:
Twenty-five male patients
who were clinically diagnosed as AKN with Fitzpatrick skin types IV (n=19),
V (n=4), and VI (n=2). Their ages ranged from 17 to 42 years .The disease
duration ranged from 5 months to 10 years. Exclusion from the study was
limited to individuals with current use of isotretinoin or previous laser
therapy. Before starting treatment patients gave their informed consent.
Patients presented with different stages of AKN; five patients presented
with papules only, three patients with keloidal lesions and seventeen
patients presented with both papules and keloidal lesions.
Laser treatment:
Each lesion was treated
with 1064nm Long-pulsed Nd: YAG laser (Cool Glide Excell; Altus Medical
Burlingam, CA) with a 10mm spot size, 35-50J/cm² fluence and 30-40 msec
pulse duration. The fluence and pulse duration differed for each patient,
dependent upon skin type and previously performed spot test. Patients with
skin type IV were treated with fluencies in the range 40- 50 J/cm² and 30
msec pulse duration while patients with skin type V and VI were treated with
lower fluencies in the range of 35- 40 J/ cm², 40 msec pulse duration. No
anaesthesia was used. Pre-cooling of the lesion was achieved by contact
cooling using the gold plated cooling head of the laser's hand piece for 3-5
seconds. The laser pulse was delivered followed by cooling for additional 2
seconds. The technique was repeated until the entire lesion was treated.
Sessions were performed monthly for six months. A lipid cream (fusidic acid
2% + betamethasone 0.1% preserved with chlorocresol) was prescribed to
patients for two to three days following each session. Sunscreen creams were
prescribed according to patients' daily activity.
Evaluation procedures:
Clinical assessments and
photographic documentation with digital camera; Kodak DX 3700, 3.1 Mega
pixels, 3xs zoom, were conducted before treatment, and repeated each session
until the end of the treatment. Patients were asked to report any adverse
effect.
Papules count:
Evaluation included papule counting at baseline that was established before
starting the laser sessions and every 2 sessions until the end of treatment.
The cut off between papule and plaque is 1 cm [10].
Keloidal plaque
size: Keloidal plaques size was determined
by measuring the width and length using a special calliper. Surface area was
then calculated and recorded in squared centimetres.
Pliability:
Keloidal plaque pliability assessment was graded according to a standard
scale to assess functional mobility of keloids and scars [11]
where 0 indicated normal skin; 1 designated supple skin that yielded with
negligible resistance; 2 indicated a yielding scar that give way to pressure
with moderate resistance; 3 designated a firm scar that moved as a solid
inflexible unit; and 4 indicated banding that produced a rope- like scar
tissue with blanching.
Evaluation was done at
baseline and every 2 sessions to the sixth session. Follow up was carried on
for 3 months.
Patient self
assessments: All patients were asked to
grade the overall percentage satisfaction with treatment one month after the
sixth session. The percentage satisfaction scale simply asked each patient
whether they were very satisfied, satisfied or not satisfied with the degree
of lesion regression by comparing pre and post treatment photos of the
lesions and symptoms alleviation as pain and pruritus.
Statistical analysis:
Mean
values were calculated for papule count, keloid size (surface area), and
pliability rating and was considered significant when the P value < 0.01.
The percentage of reduction of papule count, keloidal plaque size (area) and
pliability were defined after treatment compared to the baseline. Paired
t-test and Analysis of Variance (ANOVA) were done for comparative purpose
between mean reductions of lesions at baseline, every 2 sessions and at the
end of treatment.
Results:
Baseline
characteristics
The mean age of the patients was 27± 3.6 years (range 17- 42 years). The
mean of disease duration was 5.7± 2.1 (range 5 months -10 years). Baseline
data were 484 (range 4-56) papules, 25 keloid plaques of different sizes
(range 1-35cm²). Keloid plaques pliability was of grade 3 in eleven plaques,
grade 2 in twelve plaques and grade 1 in one plaque. Patients showed
different degrees of improvement during treatment and at the end of sessions
in papules count (fig 1a, b), keloid plaque size (fig 2a, b),
and pliability. Improvement of subjective symptoms such as pruritus, pain,
regression of lesions and cosmetic appearance were elicited. Temporary hair
loss occurred in five patients in Nd: YAG treated sites above the hair line
after the 4th session. Re- growth of thinner hair occurred 3
months after the 6th sessions in every case. Follow up period showed no
recurrence of lesions in the laser treated sites
 |
Fig 1a:
Before treatment; inflammatory papules and keloidal plaques can be
noticed. |
|
 |
Fig 1b:
After 4 sessions; improvement of both papular and keloidal plaques
with loss of hair in treated sites. |
|
 |
Fig 1c:
End of treatment regrowth of hair in the treated sites. |
|
 |
Fig 2a:
Keloidal plaque lesion before treatment. |
|
 |
Fig 2b:
Flattening of the keloidal plaque with reduction in size after
treatment. |
|
Papules count:
Significant reduction (P < 0.0001) in the mean papule count lesions after Nd:
YAG laser treatment was observed compared to the baseline (fig 3). A
31% reduction in the mean papular lesions count were observed as early as
the 2nd laser sessions with, 68.2% reduction after the 4th
laser session and 90.9 % reduction at the end of treatment.
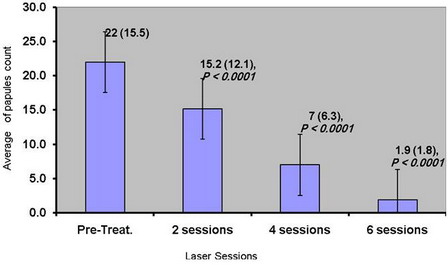 |
Fig 3:
shows reduction in mean (SD) of papules count with progress of laser
sessions. |
|
Keloidal plaque size
Significant reduction in the mean area of keloidal plaque size was initially
seen after the 4th laser session (p<0.0001) compared with the
baseline measurement (fig 4). A 5.9% reduction of keloidal plaque
size was obtained after the 2nd laser sessions, 47.1% reduction
after the 4th sessions and 70.4% reduction at the end of the treatment
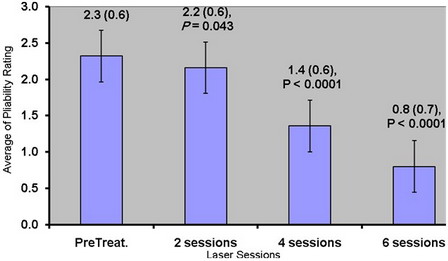 |
Fig 4:
Keloid plaque size reduction (mean ± SD) in relation to laser
sessions. |
|
Pliability
Significant keloidal plaques softening versus baseline was initially
demonstrated after the 4th laser session (p<0.0001). Progressive
reduction in pliability percentage was seen from laser session to another as
shown in (fig 5, 6). Grade 4 was not assessed in this study as it was
not present in any of the patients.
|
Fig 5:
Pliability rating progress (mean ± SD) in relation to laser
sessions. |
|
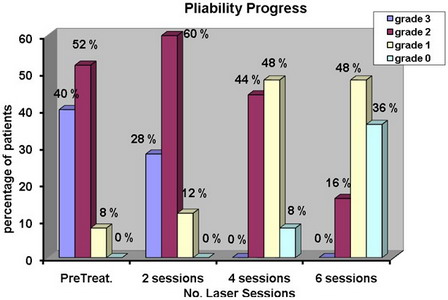 |
Fig 6:
The percentage of patients pliability improvement in relation to
Laser sessions. |
|
Subjective self
assessment:
Different degrees of satisfaction were obtained throughout sessions as shown
in table 1. By the end of 6th session, 18 patients (72%) were
very satisfied, 5 patients (38.46%) were satisfied and 2 patients (8%) were
unsatisfied.
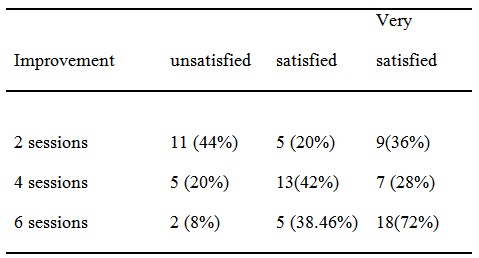 |
Table 1:
Improvement of subjective symptoms among patients (%) during
treatment |
|
Discussion:
Acne keloidalis nuchae (AKN)
is initially manifest as mildly pruritic follicular-based papules and
pustules on the nape of the neck. As folliculitis persists, keloid- like
plaques eventuate [5].
Numerous therapeutic options are available for AKN; topical and systemic
antibiotics, corticosteroids injections, surgical excisions and CO2
laser [6].
Based on the
histopathological characteristics of early lesions of AKN that show
follicular and perifollicular inflammatory infiltration at the upper third
of the hair follicle suggesting hair follicle involvement [12]
and because of the proposed similarity in causes and occasional occurrence
of pseudo- folliculitis barbae and AKN [1,13],
we decided to use the long pulsed Nd: YAG for treatment of lesions of AKN.
The 90.9% success rate in reduction in the papule count can be explained on
the basis of selective photothermolysis theory [14],
where the wavelength of long pulsed Nd: YAG laser (1064nm) penetrates far enough
into the dermis to disrupt the follicle, while sparing the epidermis from
heat absorption. This method reduces the formation of ingrown hair, thereby
reducing the severity of the disease [15,16].
Although our patients were of dark skinned type IV, V and VI, no pigmentary
changes were reported confirming that the Nd: YAG is safe for dark
skin
types [9].
The only side effect was temporary hair epilation in 5 patients due to
fragmentation and destruction of diseased follicles however, re- growth of
thinner hair was observed three months after the 6th laser
session. Shah [8]
reported marked improvement in papular and nodular AKN of three patients
treated with long pulsed diode laser 810 nm. His findings agreed with our
results however; our study was done on large sample size to improve the
ability to evaluate results. Some authors stated that keloidal lesions of
acne keloidalis is not keloid as it did not appear elsewhere in the body and
the pathology is different from that of keloid [6,12].
In keloidal plaque, distortion and occlusion of the follicular lumen by
fibrosis leads to hair retention in the inferior follicle and further
granulomatous inflammation and scarring [12].
Kanthak and Cullen [6]
were the first to emphasize the significance of sub- follicular destruction.
The reduction in the size of keloidal plaque (70.4%) after the 6th
laser session and the improvement of pliability can be explained by the
mechanism of action of long pulsed ND: YAG laser in destruction of
fragmented hairs at the inflammation site and subsequent improvement of scar
tissue.
Glenn et al., who treated
6 patients with surgical excisions, explained that lesion recurrence in 20%
of their patients was due to the incomplete removal of the ingrown hair or
new lesions formation [6].
We prescribed fusidic acid 2% with betamethasone 0.1% topical cream only for
patients who had crusts after laser sessions and for duration of 2 to 3
days, which was very short to have an influence on the clinical response. In
our study follow up for three months after the end of treatment showed no
recurrence, as the re- growing hairs were thinner and unable to re-
penetrate the skin. All patients were satisfied regarding the treatment
procedure as laser application was relatively painless on using pre cooling
technique compared to painful intra- lesional injection or surgical
excisions which require long post operative care since they are usually left
to heal by secondary intension. Improvement of pain, pruritus and cosmetic
appearance were satisfactory for all patients except two due to their high
expectations of complete cure of keloidal plaques.
Conclusion:
Treatment of AKN in early and late stages is possible and effective. By
using long pulsed Nd: YAG lasers for early papular, nodular and keloidal
lesions, satisfactory results were obtained, as being assessed by a decrease
in papular count, reduction of keloidal area as well as, the increase in
tissue pliability with no pigmentary changes. These results encourage us to
recommend this type of laser as an effective treatment modality in AKN for
dark skinned patients.References1. Dinehart SM, Herzberg AJ, Kerns BJ, et al. Acne keloidalis: a review. J Dermatol Surg Oncol 1989; 15: 642- 647.
2. Taylor SC. Epidemiology of skin disease in people of color. Cutis 2003; 71: 271-275.
3. Ogunbiyi OA, George AO. Acne keloidalis in females: case report and review of the literature. Niger J Med 2005; 97: 736- 738.
4. Smith AO, Odom RB. Pseudofolliculitis capitis. Arch Dermatol 1977; 113: 328-329.
5. George AO, Akanji AO, Nduja EU, Olasode JB, Odusan O. Clinical, biochemical and morphological features of acne keloidalis in black population. Int J Dermatol 1993; 32: 714- 716.
6. Glenn MJ, Bennett RG, Kelly AP. Acne Keloidalis Nuchae: Treatment with excision and second intension healing. J Am Acad Dermatol 1995; 33: 243- 246.
7. kantor GR, Ratz JL, Wheeland RG. Treatment of acne keloidalis nuchae with carbon dioxide laser. J Am Acad Dermatol 1986; 14: 263- 267.
8. Shah GK. Efficacy of diode laser for treating acne keloidalis nuchae. Indian J Dermatology Venerol Lepro 2005; 71(1): 31- 34.
9. Chan H, Ying SY, Ho WS, Wong DS, Lam LK. An in vivo study comparing the efficacy and complications of diode laser and long pulsed ND-YAG laser in hair removal in Chinese patients. Dermatol Surg 2001; 27(11): 950- 954.
10. James, William, Berger, Timothy, Elston, Drik (2005) Andrews' Disease of the skin: Clinical Dermatology (10th ed). Saunders. Page 16.
11. Sullivan T, Smith J, Kermode J, Mclver E, Courtemanche DJ. Rating the burn scar. J Burn Care Rehabil 1990; 11: 256- 260.
12. Herzberg AJ, Dinehart SM, Kerns BJ, Polack SV. Acne keloidalis. Transverse microscopy, immunohistochemistry, and an electron microscopy. Am J Dermatopathol 1990; 12: 109- 121.
13. Halder R. Pseudofolliculitis barbae and related disorders. Dermatol Clin 1988; 6: 407- 411.
14. Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science 1983; 22: 524- 527.
15. Ross EV, Cooke LM, Timko AL, Overstreet KA, Graham BS, Barnette DJ. Treatment of pseudofolliculitis barbae in skin types IV, V and VI with a long pulsed neodymium yttrium aluminium garnet laser. JAAD 2002 Aug; 47 (2): 263- 270.
16. Weaver SM 3rd, Sagared EC. Treatment of pseudofolliculitis barbae using long pulsed dye Nd:YAG laser on skin types V, VI. Dermatol Surg 2003; 29 (12):1187- 1191.
© 2009 Egyptian Dermatology Online Journal |
