|
|
Abstract
Sebaceous carcinoma is a rare aggressive malignant tumor derived from the adnexal epithelium of sebaceous glands. It is most commonly seen in the orbital region. Amongst extraocular sites, axilla is a very rare site of involvement. A case of rapidly growing sebaceous carcinoma of the axilla occurring in a young male with lymph node metastasis is reported. We emphasise the need to be aware of such an aggressive tumour at rare sites and the need to know the etiology better as it is no longer bound by age limits.
Introduction
Sebaceous carcinoma, which accounts for less than 1% of all cutaneous malignancies is a rare aggressive malignant tumor derived from the adnexal epithelium of sebaceous glands [1]. Orbital sebaceous carcinoma accounts for only 0.2 to 0.7 % of all eyelid tumors [2]. Despite the widespread anatomic distribution of sebaceous glands, extraorbital sebaceous carcinoma is very rare comprising only 25% of all reported cases of sebaceous carcinoma. So far only few cases of extra orbital sebaceous carcinoma are reported in the literature [1] and none in the axilla so far. Sebaceous cell carcinoma is a disease of the 6th and 7th decade of life and occurs in men and women equally [2]. Diagnosis and therapy tends to be delayed because it is frequently mistaken for more common benign entities. In addition to its varied clinical appearance, a varied histologic appearance may occur and delayed diagnosis or misdiagnosis following a biopsy is not uncommon [3]. We present a case of sebaceous carcinoma in a young male in the axilla with lymph node metastasis.
Case Report: A 32 year old male presented to the oncology clinic complaining of axillary swelling which was progressively increasing in size for the last year, rapidly enlarging in the preceding two months. Although the swelling had been largely asymptomatic, patient sought medical opinion due to its rapidly growing size and the presence of ulceration. On clinical examination, a large multinodular swelling approximately of size 5x5 cm was palpable in the right axilla. The swelling was non tender, firm, partially mobile with adherent overlying skin, which surprisingly appeared normal except for a small area of ulceration measuring 1x1 cm surrounded by erythema. Chest X ray was normal. Ultrasonography of the swelling revealed a mass of 8x6 cm suggesting a neoplastic lesion. Fine needle aspiration (FNA) was advised. FNA smears revealed clusters of and singly scattered atypical cells having round to oval nuclei with reticulo-granular chromatin, prominent nucleoli and abundant clear to vacuolated cytoplasm
(Figure 1).
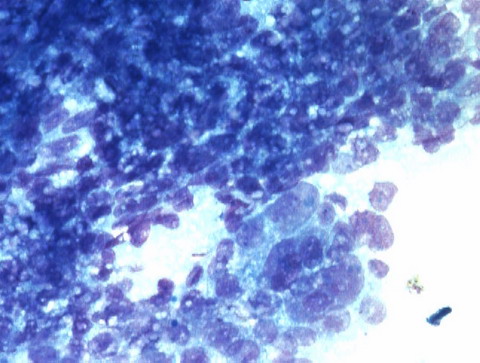 | Fig 1:
FNA smears showing cluster of atypical cells with abundant clear to
vacuolated Cytoplasm (Giemsa; X400). |
|
A diagnosis of sebaceous carcinoma was suggested and excision biopsy was performed. We received a fibrofatty nodular soft tissue mass measuring 9x7x5 cm in histopathology. Cut surface revealed grey white tumor with areas of haemorrhage and necrosis. Six lymph nodes were isolated
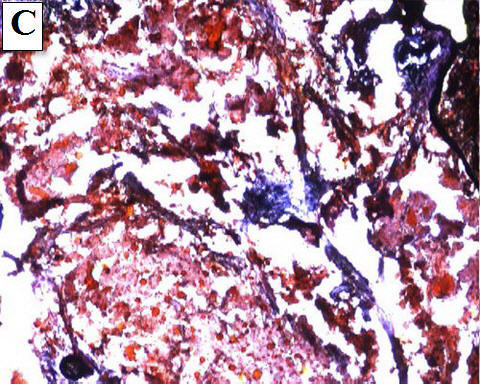
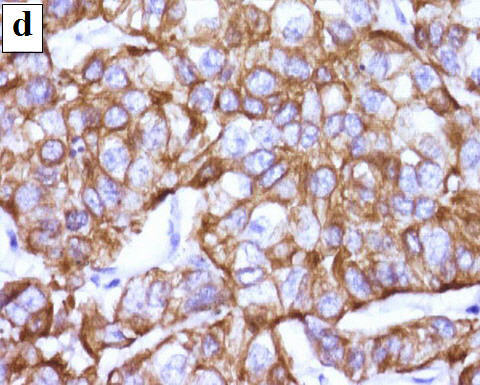
(Figure 2). Microscopic examination revealed lobules of finely vacuolated and foamy cells, separated by scant stroma. The cells had large vesicular nuclei with prominent nucleoli. Scattered mitoses were identified. Many lobules showed large central foci of necrosis. All the lymph nodes isolated showed metastatic deposits from the tumor. Periodic acid schiff (PAS) stain showed absence of any mucin. Fat stain revealed reddish lipid droplets in the cytoplasm of the cells. The tumor cells were positive for cytokeratin and epithelial membrane antigen (EMA)
(Figure 3). Thus, the diagnosis of sebaceous carcinoma was confirmed on histopathology. Patient was given external radiotherapy and chemotherapy keeping in view the young age of the patient and presence of lymph node metastases. The patient is on regular follow up for the last one and a half years and there is no evidence of recurrence and metastasis.
 | Fig
2: Excision biopsy showing grey white tumour with regional lymph
node metastasis. |
|

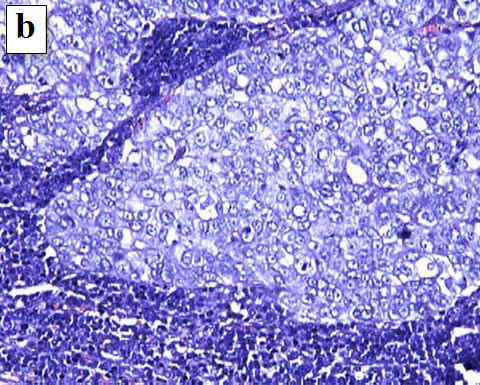
 Fig
3: Microscopic examination:
a) section showing lobules of finely vacuolated and foamy
cells, separated by scant stroma (H and E; X400),
b) metastatic tumour deposits in lymph node showing absence
of any mucin on PAS (PAS; X400),
c) fat stain revealing reddish lipid droplets in the
cytoplasm of cells (Oil red O; X200),
d) tumour cells positive for cytokeratin (CK; X400). |
|
Discussion
Sebaceous gland carcinoma is an aggressive, uncommon, cutaneous tumor first well described by Allaire in 1891. But this disease was not firmly accepted until 1956 when Straatsma thoroughly studied the histological and clinical presentation of this disease. This tumor is thought to arise from sebaceous glands in the skin and thus, may arise anywhere on the body where these glands exist [4]. It may appear on the top of pre-existing dermatoses, like nevus sebaceous and actinic keratosis or may follow radiation therapy for other diseases. It may also occur in Muir-Torre syndrome (MTS), characterized by occurrence of sebaceous tumors in association with visceral malignancies. Sebaceous carcinoma is traditionally classified into 2 groups: tumors arising from the ocular adnexa, particularly the meibomian glands and glands of zeiss, and those arising in extraocular sites. Extraocular sebaceous carcinomas most commonly involve the head and neck region, in which sebaceous glands are most plentiful, followed by external genitalia, the parotid and submandibular glands, the external auditory canal, the trunk and upper extremity, sole, the dorsum of the great toe, and laryngeal or pharyngeal cavities. The sex distribution of extraorbital sebaceous carcinoma appears to be about equal for male and female patients and the mean age of occurrence is 63 years [1]. The disease occurred in our patient at a much younger age. Histopathologically, sebaceous carcinomas are often poorly differentiated neoplasms mainly with in the dermis. Multiple lobules of basaloid undifferentiated cells are present with in dermis. In the central portion of lobules, more mature cells are present. Marked nuclear atypia, pleomorphism and mitoses are common [5]. This neoplasm may be confused with tumors composed of basal cells, squamous cells (mucoepidermoid and spindle cell carcinoma), clear and balloon nevus cells as well as other sebaceous neoplasm [6]. The histological criteria for sebaceous carcinoma are high mitotic activity, nuclear pleomorphism, lobular architecture and foamy vacoulization of the cytoplasm [2]. Histochemically, the clear cells of sebaceous carcinomas are negative with periodic acid-Schiff and Alcian blue staining. Immuno-histochemically, the tumour cells of sebaceous carcinomas show positive reactions for EMA and cytokeratin. Positivity for human milk fat globules subclass 1 & 2 (HMFG1 & HMFG2) helps to distinguish it from basal cell carcinoma [7]. The present literature is divided on the aggressive nature and metastasis potential of extraorbital sebaceous carcinoma due to its rarity and behaviour pattern. Mellette et al for instance found that the biological behaviour of extraorbital sebaceous carcinoma is not different from the orbital sebaceous carcinoma. The series by Wick, King and Hernandaz showed that distant metastases to liver, lung, bone and brain occurred in patients with extraorbital sebaceous carcinoma. Histologically the poor prognostic indicators are poor differentiation, presence of lymphatic or vascular permeation, presence of pagetoid cells shown in histology and immuno-histochemical staining [2]. Treatment of sebaceous carcinoma requires wide surgical excision with removal of regional lymph nodes. There are diverse opinions regarding the use of postoperative irradiation and chemotherapy. Metastases have been reported to occur as late as 5 years after the initial diagnosis, lending support to the continual surveillance of patients with sebaceous carcinoma [1]. Conclusion
Sebaceous carcinoma is a rare, very aggressive tumour which is generally not kept in the differential diagnosis at a site such as axilla, leading to delayed treatment. We emphasise the need to be aware of rare tumours occurring at different sites for better chances of survival of the patient. We conclude by raising the question of knowing the etiology of such aggressive tumours better, as they are no longer bound by age limits. References
1. Ghosh SK, Bandyopadhyay D, Gupta S, Chatterjee G, Ghosh A. Rapidly growing extraocular sebaceous carcinoma occurring during pregnancy: A case report. Dermatology Online Journal 2008; 14(8): 8.
2. Bhavarajua VMK, Shamim SE, Naik VR, Shaari S. Sebaceous cell carcinoma of scalp - A rare presentation. Malaysian Journal of Medical Sciences 2007; 14(1): 67-70.
3. Doxanas MT, Green WR. Sebaceous gland carcinoma. Review of 40 cases. Arch Ophthalmol 1984; 102(2): 245- 249.
4. Kass LG, Hornblass A. Sebaceous carcinoma of the ocular adnexa. Surv Ophthalmol 1989; 33(6): 477- 490.
5. Akbari D, Naraghi Z, Emadi N, Ghaninejad H. Extraocular sebaceous carcinoma arising from nevus sebaceous. Acta Medica Iranica 2005; 43(3): 227-229.
6. Kim SY, Chi JG, Lee YS. Extraocular sebaceous carcinoma - A case report. The Seoul Journal of Medicine 1987; 28(1): 47-50.
7. Mari Y, Norito I, Shoji N, Takekuni N, Osamu M, Takashi H. Two cases of extraocular sebaceous carcinoma. Nishinihon Journal of Dermatology 2000; 62(2): 199-203.© 2010 Egyptian Dermatology Online Journal |
