|
|
Abstract
Dercum's disease (adiposis dolorosa) is an unusual progressive
syndrome of unknown etiology characterized by multiple painful lipomas
that arise in adult life, most often affecting postmenopausal women who
are obese. We hereby report a case of Type III Dercum's disease in view
of the rarity of this condition.
Introduction
Dercum's disease (adiposis dolorosa) is a relatively unknown
condition which is an unusual progressive syndrome of unknown etiology
characterized by multiple painful lipomas that arise in adult life, most
often affecting postmenopausal women who are obese.[1]
Different types can be identified according to the spread of pain:
o Type I, or the juxta- articular type,
o Type II, or the diffuse, generalized type,
o Type III, or the lipomatosis, nodular type, with pain in and around
multiple lipomas, sometimes in the absence of general obesity; lipomas
are approximately 0.5-4 cm, soft, and attached to the surrounding
tissue. We report this case because of the rarity of the disease.
Case Report
A 37 year old married normotensive non-obese (weight = 45 kgs) woman
from Drass Kargil reported to the outpatient department of Dermatology,
STD and Leprosy of Government Medical College Srinagar with 9 years'
history of multiple, nodular, painful sub-cutaneous swellings
symmetrically distributed mainly over both forearms with few lesions
over thighs and lower back. These swellings first appeared in the left
forearm with a single lesion which progressively increased in size with
the appearance of similar lesions over the other arm. Hyperalgesia was
found in the fatty tissue below the skin on light pressure and touch
with exacerbation on exposure to cold and on exertion. Pain did not
increase in connection with menstruation and menstrual cycles were
normal. There is history of paresthesias and swelling of hands. There is
no history of morning stiffness, tiredness, headache, depression, loss
of sleep and appetite or bruising tendency. There is no history of any
menstrual irregularities, oral contraceptive bills use or intake of oral
steroids. There is a similar history of painful subcutaneous swellings
over forearms in her elder brother. No other significant relevant
history present.
On examination; multiple, tender, freely mobile, soft to firm in
consistency, sub-cutaneous nodules of sizes varying from 0.5- 7cm were
seen on both forearms on both extensor and flexor aspects. These
swellings were not adherent to the overlying skin which did not show any
surface changes. Similar lesions were seen on the thighs and lower back.
(Figs 1, 2 and 3)
 | Fig 1:
Multiple subcutaneous swellings over flexor aspects of both
forearms. |
|
 | Fig
2: Multiple subcutaneous swellings over extensor aspect of
both forearms. |
|
 | Fig
3: Multiple subcutaneous swellings over the back. |
|
Routine investigations on blood including complete blood count,
liver, kidney and thyroid function tests were within normal limits.
Coagulation tests and erythrocyte sedimentation rate were also within
normal limits. Lipid profile, fasting blood sugar, alpha-1 antitrypsin,
complement levels- C3 and C4 levels were also within normal limits. Fine
needle aspiration cytology (FNAC) revealed the lipomatous origin of
these lesions with normal capsule formation. (Fig 4)
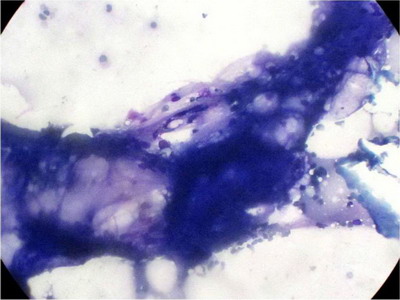 | Fig
4: FNAC showing the lipomatous nature of the lesion. |
|
On the basis of typical clinical features and investigations in this
non-obese female a diagnosis of Type III Dercum's disease was made.
Discussion
Dercum's disease was first described in 1892 by the American
neurologist Francis Xavier Dercum. Dercum's disease is believed to be
transmitted in an autosomal dominant manner [2,3],
however most reported cases of adiposis dolorosa are sporadic.[4]
The understanding of the pathogenesis and the mechanism of Dercum's
disease remain unknown. It is believed that fatty deposits cause nerve
compression and result in weakness and pain.
Dercum's disease (adiposis dolorosa) is rare and is 20 times more
common in females who are postmenopausal, obese, or overweight than in
other people. However, it can occur in individuals who are not obese. It
usually occurs in persons aged 45-60 years. Rarely, it occurs in women
younger than 45 years. Adiposis dolorosa is almost never seen in
children. Previously healthy women notice lumps or previously present
lumps start growing. They describe pain and discomfort in the region of
the lumps associated with weakness. Before the onset of the disease, the
patient is usually only slightly obese, but, in a short time, the
patient becomes overweight. Hyperalgesia is found by light pressure and
touch in the fatty tissue below the skin and is made worse by tightly
fitting clothes or showering. The pain is temperature and weather
dependent. Other symptoms include swelling of fingers, general
tiredness, tendency to bruise with normal coagulation tests, morning
stiffness, headaches, cognitive dysfunction and bouts of depression.
Results of hormonal studies to rule out Cushing syndrome, thyroid
abnormalities, and other endocrinologic abnormalities are normal in
patients with Dercum's disease (adiposis dolorosa) however they might
have associated slight-to-moderate rises of cholesterol levels.
Erythrocyte sedimentation rate results can be slightly elevated.
Coagulation test results are normal. In spite of obesity, hypertension
and type 2 diabetes mellitus seldom occur. An increase in certain active
parameters may be seen in the following: sedimentation rate;
alpha-1-antitrypsin; orosomucoid (alpha-1-acid glycoprotein, an acute
phase reactant); haptoglobin; and complement factors C3, C4, Clq, and
Cls. [5,6]
A review of histopathologic findings did not reveal any significant
features that might distinguish Dercum's disease (adiposis dolorosa)
tumors from the common sporadic lipomas. The tumors can be encapsulated,
or the fatty deposits can be diffuse.
Traditional management of Dercum's disease has been largely
unsatisfactory relying on weight reduction and surgical excision of
particularly troublesome lesions.
Non-pharmacological approaches for Dercum's disease (adiposis
dolorosa) may be used as adjuncts to pharmacologic treatments. Some of
these include acupuncture, cognitive behavioral therapy, hypnosis, and
biofeedback. [4]
Pharmacological treatments include Prednisolone, [7],
intravenous lidocaine [8,9],
NSAIDS, diuretics, INF alpha, oral mexiletine [9]
and infliximab [10]. Surgical
management includes liposuction and surgical excision of isolated
painful lipomas.
Dercum's disease usually occurs in obese post-menopausal middle-aged
women but here we report a case of Type III Dercum's disease in a 37
year old non-obese woman.
References
1. Dercum FX. Three cases of a hitherto unclassified
affection resembling in its grosser aspects obesity, but associated with
special symptoms: adiposis dolorosa. Am J Med Sci. 1892; 104: 521- 35.
2. Lynch HT, Harlan WL. Hereditary Factors in Adiposis
Dolorosa (Dercum's Disease). Am J Hum Genet. Jun 1963; 15(2): 184- 90.
3. Cantu JM, Ruiz-Barquin E, Jimenez M, Castillo L,
Macotela-Ruiz E. Autosomal dominant inheritance in adiposis dolorosa
(Dercum's disease). Humangenetik. Mar 23 1973; 18(1): 89- 91.
4. Campen R, Mankin H, Louis DN, Hirano M, Maccollin M.
Familial occurrence of adiposis dolorosa. J Am Acad Dermatol. Jan 2001;
44(1): 132- 6.
5. Greenbaum SS, Varga J. Corticosteroid-induced
juxta-articular adiposis dolorosa. Arch Dermatol. Feb 1991; 127(2): 231-
3.
6. Skagen K, Petersen P, Kastrup J, Norgaard T. The
regulation of subcutaneous blood flow in patient with Dercum's disease.
Acta Derm Venereol. 1986; 66(4): 337- 9.
7. Palmer ED. Dercum's disease: adiposis dolorosa. Am
Fam Physician. Nov 1981; 24(5): 155- 7
8. Iwane T, Maruyama M, Matsuki M, Ito Y, Shimoji K.
Management of intractable pain in adiposis dolorosa with intravenous
administration of lidocaine. Anesth Analg. Mar-Apr 1976; 55(2): 257- 9.
9. Petersen P, Kastrup J. Dercum's disease (adiposis
dolorosa). Treatment of the severe pain with intravenous lidocaine.
Pain. Jan 1987; 28(1): 77- 80.
10. Singal A, Janiga JJ, Bossenbroek NM, Lim HW.
Dercum's disease (adiposis dolorosa): a report of improvement with
infliximab and methotrexate. J Eur Acad Dermatol Venereol. May 2007;
21(5): 717.© 2012 Egyptian Dermatology
Online Journal
|
