|
|
Abstract
Erythromelanosis follicularis faciei et colli (EFFC), characterized by
hyperpigmentation, erythema and follicular papules on face and neck, is
a rare disease and not previously reported from Nepal. We report a case
of 13 years old boy who presented with classical triad of EFFC and present
a literature review on this condition.
Case report
A 13 years old boy presented with redness, pigmentation and raised rough
lesions on the face since early childhood. He recognized an increase in
the erythema and burning sensation on exposure to light. He denied any similar
history in his family. Physical examination revealed follicular papules,
erythema and hyperpigmentation present on the malar area, which was bilaterally
symmetrical extending to the pre-auricular area, ear lobules and neck as
shown in Figure 1 and Figure 2. There was no atrophy, scarring or alopecia.
Systemic examination failed to reveal any significant abnormality. Patient
was put on topical tretinoin 0.025% cream, emollients and sunscreen. Patient
denied for skin biopsy. On follow up over 1 month his symptoms remain static.
 | Fig 1:
follicular papules, erythema and hyperpigmentation seen in malar
area, preauricular and ear lobules. |
|
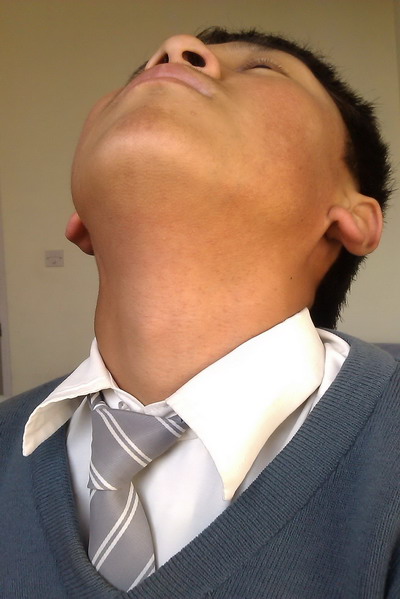 | Fig
2: Extension of the follicular papules, erythema and
hyperpigmentation on the neck |
|
Discussion
Erythromelanosis follicularis faciei et colli (EFFC) is a disorder of
unknown etiology which classically presents with a triad of hyperpigmentation,
erythema (with or without telangiectasia) and follicular papules on the
pre-auricular and cheek areas. Our case is also a classic presentation of
EFFC. Initially coined by Kitamura in 1960, EFFC is a rare disease and only
55 cases are reported in the literature. Common age of presentation is adolescence
and preferably seen in males [1,2,3].
EFFC also affects children and young adults. There have been many reports
of EFF in women since last two decades [4,5].
Bilateral distribution is the main characteristic but unilateral cases were
described [1]. Clinical presentations of
most reported cases are similar. However, there are variations in symptoms
and seasonal influences [4,6].
Our case also had exaggeration of symptoms on photo exposure. EFFC emerge
sporadically, however, there are reports of cases people from the same family.
The disease may have an autosomal recessive mode of inheritance as reported
by Yanez et al [7,8].
EFFC has recently been considered to be a poly-etiological disorder with
the possibility of a chromosomal instability syndrome [4].
Histopathology though not diagnostic, shows follicular plugging, hyperkeratosis,
increase pigmentation in the basal membrane, perivascular and periadnexal
inflammatory infiltrate and follicular dilatation [1].
Differential diagnoses include athrophoderma vermiculatum, ulerythema ophryogenes
and poikiloderma of Civatte. Keratosis pilaris is known to be associated
with EFFC [4,9].
Treatment so far is unsatisfactory. Topicals like ammonium lactate 12%,
tretinoin cream (0,050,1%), salicylic acid 2%, metronidazole and combinations
with hydroquinone 4% has been tried, so is chemical Peel with salicylic
acid (30%) [1,5,10].
In severe cases oral isotretinoin is used intermittently. Pulsed Dyed Laser
of 595nm is a newer therapeutic option to attenuate hyperpigmentation and
erythema [1].
Conclusion
Erythromelanosis follicularis faciei et colli (EFFC), is a disorder of
unknown etiology classically present with a triad of hyperpigmentation,
erythema (with or without telangiectasia) and follicular papules on face
and neck. Treatment till date is not satisfactory. Rarity of this condition
demands more case description to characterize the disease. We report this
classic case for the first time in Nepal.
References
1. Da silva R.S, Fonseca J.C.M, Obadia D. Case for diagnosis.
Anais Brasileiros de Dermatologia . 85(6):923-925, 2010.
2. Sardana K, Relhan V, Garg V, Khurana N. An observational
analysis of erythromelanosis follicularis faciei et colli. Clin Exp Dermatol.
33:333-6, 2007.
3. Ermertcan AT, Oztürkcan S, Sahin MT, Türkdogan P, Saçar
T. Erythrodermelanosis follicularis faciei et colli associated with keratosis
piaris in two brothers. Pediatr Dermatol.23:31-34,2006.
4. Augustine M, Jayaseelan E. Erythromelanosis follicularis
faciei et colli: Relathionship with kertaosis pilaris. Indian J Dermatol
Venereol Leprol. 74:47-49, 2008.
5. Ertam I, Unal I, Alper S. Erythromelanosis follicularis
faciei et colli: report of involvement in two female patients. Dermatol
Online J.;11(2):23, 2005.
6. Sodaify M, Baghestani S, Handjani F, Sotoodeh M. Erythromelanosis
follicularis facie et colli. Int J Dermatol. 33:643-4, 1994.
7. Yanez S, Velasco JA, Gonzalez MP. Familial erythromelanosis
follicularis et colli-an autosomal recessive mode of inheritance. Clin Exp
Dermatol. 18(3);283-5. 1993.
8. Acay MC. Erythromelanosis follicularis faciei et colli.
A genetic disorder? Int J Dermatol. 32(7);542, 1993.
9. Gupta Lalit, Garg Anubhav, Khare Ashok Kumar, Mittal
Asit Familial erythromelanosis folicularis faciei et colli with extensive
keratosis pilaris . International Journal of Dermatology. 50(11): 1400,
2011.
10. Kim WJ, Song M, Ko HC, Kim BS, Kim MB. Topical tacalcitol
ointment can be a good therapeutic choice in erythromelanosis follicularis
faciei et colli. J Am Acad Dermatol. 67(2):320-1,2012.
© 2013 Egyptian Dermatology Online Journal
|
