|
|
Abstract
The frequency of cutaneous metastasis is estimated at 4% of visceral
cancers. They are rarely indicative of extra-dermatologic cancers, however,
recognizing a cutaneous metastasis or paraneoplastic dermatosis can be of
great diagnostic and / or prognostic value. We report a 51 year old patient
presented with cutaneous metastasis indicative of a pulmonary
adenocarcinoma. She received radiotherapy combined with chemotherapy without
remission and died after five months. Introduction
Cutaneous metastasis frequency is estimated at 4% of visceral cancers [1].
The lung cancer and breast cancer are the commonest providers of cutaneous
metastasis [2]. Among lung cancers, large
cell carcinoma is the one that accompanies most cutaneous metastasis,
followed by adenocarcinoma. We report a patient with poorly differentiated
pulmonary adenocarcinoma, which was revealed by cutaneous metastasis
associated with liver, adrenal, bone and soft tissue metastasis. Case
report
A 51- year-old woman was admitted with subcutaneous nodules, asthenia,
anorexia, weight loss and fever of 38.5° C. The symptoms had been present
for one month. The physical examination at admission revealed multiple
subcutaneous nodules involving the back and trunk, firm without signs of
inflammation (Fig 1) and enlarged liver (liver metastasis).
 | Fig 1:
Subcutaneous nodules, firm, very limited, affecting the back and
trunk. |
|
Laboratory tests showed biological inflammatory syndrome (erythrocyte
sedimentation rate = 80 mm in the first hour and C-reactive protein=60mg/l).
Sputum and urine tests were negative for the tuberculosis bacillus, as well
as urine culture and viruses serology (HIV, B and C hepatitis) were
negative. Chest radiography showed a left retrocardiac opacity. A nodule
excisional biopsy was performed and histology showed a dermis and hypodermis
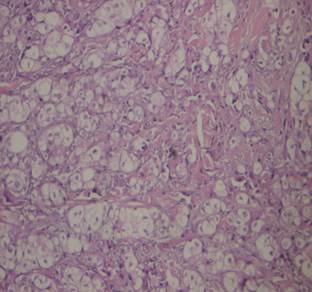
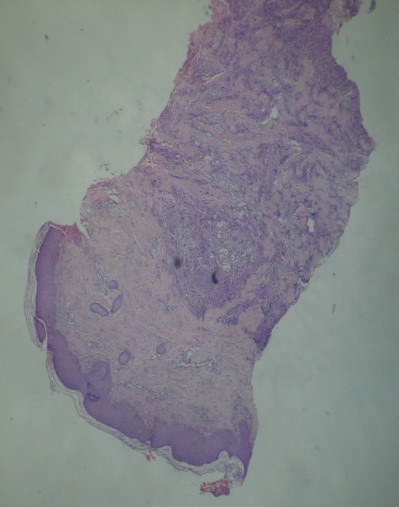
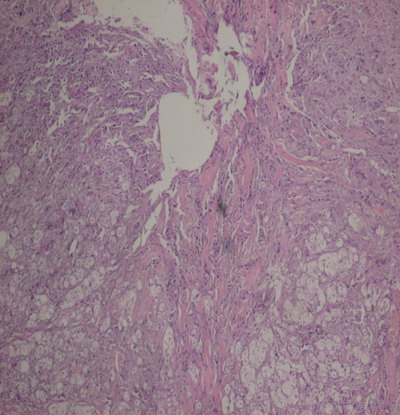
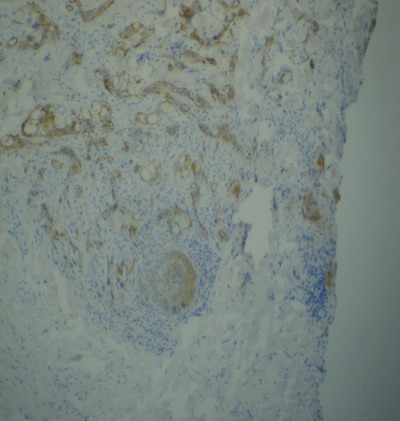
infiltrated by a carcinomatous proliferation (Fig 2,3,4,5). The
diagnosis of cutaneous metastasis was chosen and a series of additional
investigations were undertaken in search of a primary tumor.
Fig 2, 3, 4,5: Diffuse infiltration of the dermis and hypodermis
by a cancerous proliferation of cells made with abundant, clear and
eosinophils cytoplasm . The nuclei are atypical. Tumor cells express
cytokeratin.
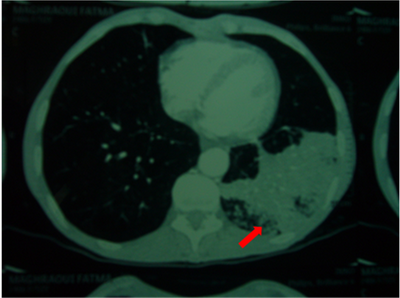
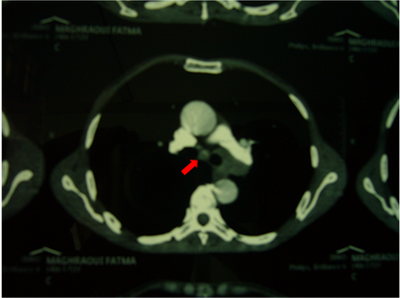
The CT scan
revealed a left bilobar pulmonary mass associated with homo and
contralateral lymph nodes, liver, adrenal, bone and parts soft tissue
metastasis (Fig 6,7).
Fig 6,7: Left bilobar pulmonary mass associated with homo and
contralateral lymph nodes. Bronchoscopy showed an inflammatory and
thickened left main bronchus and its terminal portion. The orifice of the
left lower lobe bronchus was not catheterisable. The left upper lobe
bronchus is reduced in size. The mucosa is hemorrhagic. Trans-bronchial
biopsy was performed and histological examination confirmed the presence of
a poorly differentiated adenocarcinoma. This patient's cancer was classified
T4N2M1b and the patient was proposed for palliation treatment. She received
radiotherapy combined with chemotherapy without remission, and she died
after five months. Discussion
Cutaneous manifestations of cancer, rarely revealing extra skin cancers
are of two types: Paraneoplastic dermatosis and cutaneous metastasis.
Paraneoplastic dermatosis do not have the malignancy characters and the
development is parallel to the tumor. The cutaneous metastasis, in
contrast, have a dermal or subcutaneous tumor growth made of extra skin
malignant cells. The skin is normally considered an infrequent site of deep
cancers metastatic [3]. Cutaneous metastasis
frequency is estimated at 4% of visceral cancers [1].
The lung cancer and breast cancer are the most providers of cutaneous
metastasis [2]. According to data from the
literature between 0.9% and 8.7% of patients with lung cancer have developed
cutaneous metastasis [4-7].
Skin metastasis may be indicative of the disease in 0.19% of cases [7],
which was the case with our patient. Among lung cancers, large cell
carcinoma is the one that provides most cutaneous metastasis, followed by
adenocarcinoma, small cell lung cancer and squamous cell carcinoma
respectively. Clinically, the cutaneous metastasis most often presents one
or more subcutaneous nodules which are hard, mobile, covered with normal or
inflammatory skin, and are usually painless. They vary in size from a few
millimeters to several centimeters. The spontaneous evolution is towards
necrotic ulceration with frequent super-infection. Sometimes it is a
carcinomatous lymphangitis, erythematous closet, occurring in the cutaneous
territory next to the primary tumor [4]. The
presence of cutaneous metastasis is usually an advanced evolutionary stage
of cancer [8] since it is frequently
associated with other metastasis. In the case of our patient, the cutaneous
metastases were associated with liver, adrenal, bone and soft tissue
metastasis. The treatment of cutaneous metastasis when they are small and
few in number may be covered by surgical excision or radiotherapy if the
tumor is radiosensitive. Unresectable metastasis can sometimes benefit from
palliative radiotherapy to analgesic. The indication for chemotherapy
follows the regimens specific to the primary tumor. Conclusion
Any skin lesion that has not proven its etiology should be investigated
for a neoplastic affection. Histological study allows rapid orientation and
avoids the diagnosis and therapy delay References
1. Brownstein MH, Helwig EB. Spread of tumors tothe skin. Arch Dermatol
1973; 107: 80-6.
2. Brownstein MH, Helwig EB.
Metastatic tumors of the skin. Cancer 1972; 29: 1298-307.
3. Kanitakis J. Les métastases cutanées des cancers profonds. Presse Méd
1993 ; 22 : 631-6.
4. Terashima T, Kanazawa M. Lung
cancer with skin metastasis. Chest 1994;106:1448–50.
5. Kamble R, Kumar L, Kochupillai V, Sharma A, Sandhoo MS, Mohanti BK.
Cutaneous metastases of lung cancer. Postgrad med J 1995;71:741–3.
6. Hidaka T, Ishii Y, Kitamura S. Clinical features of skin metastasis from
lung cancer. Intern Med 1996; 35:459– 62.
7. Triller
Vadnal K, Triller N,
Požek
I, Kecelj P,
Košnik
M. Skin metastases of lung cancer. Acta Dermato venerol Alp Panonica Adriat
2008; 3: 125-8.
8. Haddad A, Sahli A, Njim L, Essid
A, Denguezli W,Zakhama A. Métastase cutanée gigantesque d'un carcinome
mammaire. La Tunisie Medicale 2011; 03: 310-311.
© 2013 Egyptian Dermatology Online Journal |