|
|
Abstract
Background: Possible relationship between dermatoglyphic patterns and other diseases, including dermatological diseases, especially those with genetic and hereditary basis such as vitiligo, psoriasis, alopecia areata, have been found in various studies but there is paucity of data from India to uphold the association.
Aims and Objectives: To study the relationship between dermatoglyphic patterns with various dermatoses such as psoriasis, vitiligo, alopecia areata, and pemphigus vulgaris.
Material and methods: This hospital based study involved 140 patients with psoriasis, 76 with vitiligo, 84 with alopecia areata and 30 pemphigus vulgaris patients, compared to 1838 age and sex matched control patients. Rolled finger and hand prints of palmar surfaces of both hands were obtained by the ink method.
Results and observations: In the control group, loop pattern of dermatoglyphics was the commonest, found in 54.52%, followed by whorls in 36.78% and arch in 8.70%. In psoriasis patients, whorl pattern was the commonest (44.29%), followed by 31.43% loop, 21.43% arch and 2.86% composite pattern. In vitiligo patients, loop and whorl pattern was found in 44.74% patients each, followed by arch pattern in 10.53%. In patients of alopecia areata, whorl pattern was found in 45.24% patients followed by loop in 30.95% and arch pattern in 23.81% while in pemphigus vulgaris patients, loop pattern was found in 50% patients, followed by whorl in 40% and arch in 10% patients.
Conclusion: There was statistically significant difference between psoriasis patients and controls regarding loop, arch and composite patterns, but no significant difference with respect to whorl pattern. Similarly, there was a significant difference between alopecia areata patients and controls for loop and arch patterns, but no significant difference regarding whorl pattern. There was, however, no significant difference regarding any of the dermatoglyphic patterns between vitiligo and pemphigus vulgaris patients and controls. Introduction
Scientific study of the epidermal ridges and their configuration on the volar aspect of hands, fingers, feet and toes is called dermatoglyphics. Derived from Greek word derma = "skin", and glyph = "carving", dermatoglyphics can be traced back to 1892 when biologist Sir Francis Galton, published his classic work on fingerprints. The study was later termed dermatoglyphics by Dr. Harold Cummins, the father of American fingerprint analysis.[1] The epidermal ridges are usually laid down between the tenth and eighteenth weeks of gestation. Once laid down, they remain unchanged except for an increase in size in parallel with general growth.[2,3,4] Dermatoglyphic patterns may be of great value for genetic studies as they are not influenced by age, postnatal environmental factors, nor are they subject to any influences in the later prenatal period.[5] Whenever there is any abnormality in the genetic makeup of parents, it is inherited by the children and reflected in dermatoglyphic pattern. Hence the study of dermatoglyphics had been proven to be of great use in predicting the possibility of inheriting hereditary disease in patients.[6,7] In clinical medicine, chromosomal anomalies such as Patau's syndrome, Edwards' syndrome, Down's syndrome, Turner's syndrome, Kleinfelter's syndrome, Cri du Chat syndrome are recognized as having abnormal dermatoglyphic patterns.[8,9] Differences in fingerprint pattern frequencies from normal controls have also been found in leukaemia, early onset diabetes mellitus, atopic dermatitis, rubella embryopathy, chronic intestinal pseudo obstruction, rheumatoid arthritis and idiopathic dilated cardiomyopathy.[10,11,12,13] Dermatoglyphics as a diagnostic tool is well established in a number of other diseases having strong hereditary or genetic basis.[14,15,16,17,18,19,20,21,22] These observations suggested that hereditary or environmental factors acting in early gestation may have played a role in the genesis of the disease.[23,24,25,26,27] This encouraged us to revisit this forgotten subject and share our experience with the study of dermatoglyphic patterns in psoriasis, vitiligo, alopecia areata and pemphigus vulgaris. These diseases were selected because of known genetic and hereditary basis for their occurrence.[28] Material and methods
In this prospective hospital based case control study, the study group comprised patients of psoriasis, vitiligo, alopecia areata and pemphigus vulgaris, diagnosed clinically and histopathologically at times, taken up for the study after a written informed consent, over a period of one year. Patients above the age of 12 years were recruited for the convenience of obtaining finger prints. Rolled finger and hand prints of palmar surfaces of both hands were obtained by the ink method as suggested by Cummins and Midlo.[1] This was done by asking the subjects to clean their hands with soap and water and then dry them up leaving behind slight moisture. A requisite amount of ink was placed on a glass slab and uniformly smeared by a rubber roller to get a thin and even film. The expanded palms were placed on the ink film coated glass slab and slight pressure applied on the dorsum of hands and digits, so that the hollow of the palms and flexor creases over palms and fingers get uniformly inked. The inked hands of the subjects were pressed on a sheet of white paper from proximal to distal end. The palm was then lifted away from the paper in reverse order from distal to proximal end. The fingers were rolled from radial to ulnar side to obtain a complete impression of the ball of the finger. The prints were subjected to detailed digito-palmar dermatoglyphic analysis with the help of magnifying hand lens, and qualitative analysis was done regarding various dermatoglyphic patterns. Only the major types of fingerprint patterns were identified, including arch, loop, whorl, and composite, the diagrammatic representation of which is shown in figure 1.
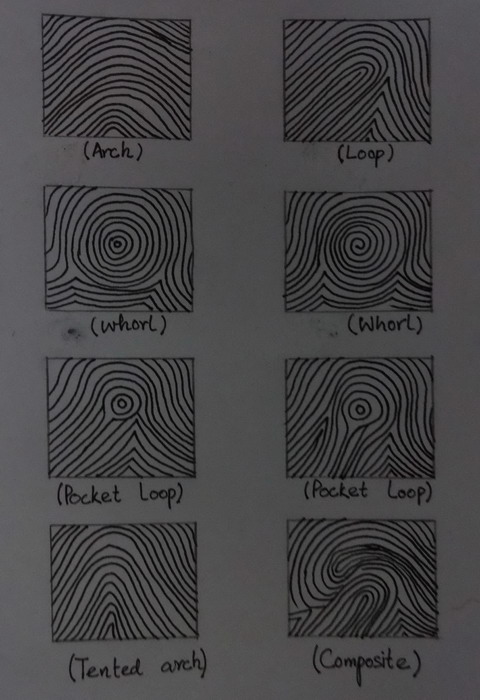 | Fig 1:
Diagrammatic representation of major dermatoglyphic patterns |
|
The results in the study group were compared with the control group which comprised of randomly selected age and sex matched patients visiting the dermatology department for other dermatological diseases. The data was compiled and subjected to statistical analysis using software SPSS version 16, using chi square (ϒ2) test and taking p value of <0.05 as significant. Results
The study group involved 140 patients with psoriasis, 76 with vitiligo, 84 with alopecia areata and 30 pemphigus vulgaris patients. The control group comprised of dermatoglyphics from 1838 age and sex matched patients visiting for other dermatoses. Out of 1838 control patients, loop pattern of dermatoglyphics was the commonest, found in 1002 (54.52%), followed by whorls in 676 (36.78%) and arch in 160 (8.70%) patients. Out of 140 patients of psoriasis, 98 (70%) were males and 42 (30%) females, with male to female sex ratio of 2.3: 1. The age of psoriasis patients ranged from 13 years to 70 years, with average age of 32.8 years. There were 76 patients (54.29%) in the age group 21-40 years, 32 (22.86%) in the age group 13-20, and 32 (22.86%) in the age group
≥ 41 years. There were 98 patients (70%) from rural background and 42 (30%) from urban. The duration of the disease ranged from 10 days to 30 years, with an average disease duration of 6.24 years. 94 patients presented with psoriasis vulgaris, 18 with scalp psoriasis, 16 with guttate type, 8 with erythroderma, and 4 with pustular type of psoriasis. Whorl pattern of dermatoglyphics was found in 62 (44.29%) patients of psoriasis, 48 males and 14 females. 44 (31.43%) patients had loop pattern, 28 males and 16 females. Arch pattern was found in 30 patients (21.43%), 20 males and 10 females, and composite pattern in 4 (2.86%) patients, 2 each from males and females. There was statistically significant difference between psoriasis patients and controls regarding loop, arch and composite patterns, but no statistically significant difference with respect to whorl pattern. Of the 76 patients of vitiligo, 42 (55.26%) were males and 34 (44.74%) females, with male to female sex ratio of 1.2: 1. The age of vitiligo patients ranged from 13 years to 45 years, with average age of 23.47 years. There were 44 (57.89%) patients in the age range 21-40 years, 30 (39.47%) in 13-20 years, and 2 (2.63%) in the age group of
≥ 41 years. Six patients had positive family history of vitiligo. There were 44 (57.89%) patients from rural areas and 32 (42.11%) from urban background. The duration of disease ranged from 2 months to 15 years, with average disease duration of 4.89 years. Fifty- eight patients had diffuse involvement, 10 focal, 4 acral type, 2 had acrofacial and 2 had generalized type of vitiligo. Loop pattern was found in 34 (44.74%) patients of vitiligo, 20 females and 14 males. Thirty- four (44.74%) patients; 18 males and 16 females, had whorl pattern while 8 (10.53%) patients had arch pattern; 6 females and 2 males. There was, however, no statistically significant difference regarding any of the dermatoglyphic patterns between vitiligo patients and controls. Eighty- four patients of alopecia areata were included in the study including 56 (66.67%) males and 28 (33.33%) females, with male to female sex ratio of 2: 1. The age of alopecia areata patients ranged from 13 years to 50 years, with average age of 25.93 years. There were 64 (76.19%) patients in the age group 21-40 years, 18 (21.43%) in 13-20 years, and 2 (2.38%) in the age group
≥ 41 years. Fifty- two (61.90%) patients had rural background and 32 (38.10%) had urban background. The disease duration ranged from 8 days to 4 years, with an average disease duration of 4.29 months. Eighty patients presented with localized disease, and 2 had diffuse and 2 had ophiasis types of alopecia. Whorl pattern of dermatoglyphics was found in 38 (45.24%) patients of alopecia areata; 26 males and 12 females while 26 (30.95%) patients had loop pattern, comprising of 18 males and 8 females. Arch pattern was found in 20 (23.81%) patients; 12 males and 8 females. There was a statistically significant difference between alopecia areata patients and controls with respect to loop and arch patterns, but no significant difference regarding whorl pattern. Thirty patients of pemphigus vulgaris studied comprised of 18 (60%) males and 12 (40%) females, with a male to female sex ratio of 1.5:1. The age of pemphigus vulgaris patients ranged from 33 years to 65 years, with average age of 49.6 years. Twenty- one (70%) patients were in the age group of
≥ 41 years and 9 (30%) in 21-40 years age group. There were 27 (90%) patients from rural areas and 3 (10%) from urban areas. Eighteen patients presented with cutaneous and 12 with mucocutaneous involvement. The disease duration ranged from 1 month to 15 months, with an average duration of 7.4 months. Loop pattern was found in 15 (50%) patients of pemphigus vulgaris; 9 females and 6 males while 12 (40%) patients; 9 males and 3 females, had whorl pattern. Three (10%) patients, all males had arch pattern of dermatoglyphics. There was no statistically significant difference between pemphigus vulgaris patients and controls with respect to any of the dermatoglyphic patterns studied. The demographic variables of the study group and the dermatoglyphic patterns between cases and controls are summarized in
tables 1 and 2, respectively. Some of the actual images of the dermatoglyphic patterns in our patients are shown in
figure 2.
|
|
|
Psoriasis |
Vitiligo |
Alopecia areata |
Pemphigus vulgaris |
|
Sex distribution |
Males |
98 |
34 |
56 |
18 |
|
Females |
42 |
42 |
28 |
12 |
|
Total |
140 |
76 |
84 |
30 |
|
Male: Female sex ratio |
2.3:1 |
1.2:1 |
02:01 |
1.5:1 |
|
Age distribution |
13-20 years |
32 |
30 |
18 |
0 |
|
21-40 years |
76 |
44 |
64 |
9 |
|
≥41 years |
32 |
2 |
2 |
21 |
|
Average age (years) |
32.8 |
23.47 |
25.93 |
49.6 |
|
Residential distribution |
Rural |
98 |
44 |
52 |
27 |
|
Urban |
42 |
32 |
32 |
3 |
|
Average duration of disease |
|
6.24 years |
4.89 years |
4.29 months |
7.4 months |
Table 1: Demographic variables in the study group
|
|
|
Psoriasis (n=140) |
Vitiligo (n=76) |
Aloecia areata (n=84) |
Pemphigus vulgaris (n=30) |
Control (n=1838) |
p value |
|
Loop |
Total |
44 |
34 |
26 |
15 |
1002 |
Ps:0.000 (S) |
|
Vit:0.119 |
|
AA:0.000 (S) |
|
Males |
28 |
14 |
18 |
6 |
|
PV:0.758 |
|
Females |
16 |
20 |
8 |
9 |
|
|
|
Whorl |
Total |
62 |
34 |
38 |
12 |
676 |
Ps:0.093 |
|
Vit:0.198 |
|
AA:0.146 |
|
Males |
48 |
18 |
26 |
9 |
|
PV:0.863 |
|
Females |
14 |
16 |
12 |
3 |
|
|
|
Arch |
Total |
30 |
8 |
20 |
3 |
160 |
Ps:0.000 (S) |
|
Vit:0.732 |
|
AA:0.000 (S) |
|
Males |
20 |
2 |
12 |
3 |
|
PV:0.939 |
|
Females |
10 |
6 |
8 |
0 |
|
|
|
Composite |
Total |
4 |
0 |
0 |
0 |
0 |
Ps:0,000 (S) |
|
Vit: 0 |
|
AA: 0 |
|
Males |
2 |
0 |
0 |
0 |
|
PV: 0 |
|
Females |
2 |
0 |
0 |
0 |
|
|
Ps= Psoriasis, Vit=Vitiligo, AA= Alopecia
areata, PV= Pemphigus vulgaris
Table 2. Dermatoglyphic patterns in the
study and control groups
 | Fig
2:
Actual dermatoglyphic patterns on the patients |
|
Discussion
In this study, loop pattern of dermatoglyphics was the commonest pattern in the control group, found in 54.52%, followed by whorls in 36.78% and arch in 8.70%. This is in accordance with the higher percentage of loop pattern in the normal individuals found in the literature. In our study, in psoriasis patients, whorl pattern was the commonest (44.29%), followed by 31.43% loop, 21.43% arch and 2.86% composite pattern. Furthermore, there was statistically significant difference between psoriasis patients and controls regarding loop, arch and composite patterns, but no statistically significant difference with respect to whorl pattern. In a previous study by Kapur et al, increased loop and decreased whorls were seen, which is in contrast to the results of our study.[25] We could not lay our hands on other studies in the literature, in order to compare our results regarding psoriasis. In vitiligo patients in our study, loop and whorl pattern was found in 44.74% patients each, followed by arch pattern in 10.53%, but there was no statistically significant difference regarding any of the dermatoglyphic patterns between vitiligo patients and that in controls. In a previous study by Sumit Kar et al, increased loops and arches, and decreased whorls were found in 112 patients of vitiligo.[29] Singh et al also found loop pattern being more common.[30] Decreased percentage of whorls was also noted in other studies.[30,31,32] Increased percentage of total arches in female vitiligo patients was reported by Iqbal et al.[24] The results of some of these studies are in contrast to that of ours. In patients of alopecia areata in our study, whorl pattern was found in 45.24% patients followed by loop in 30.95% and arch pattern in 23.81%, and there was a statistically significant difference between alopecia areata patients and controls with respect to loop and arch patterns, but no significant difference regarding whorl pattern. Statistically significant increased loop pattern were also found in some previous studies.[33] Similarly, increased arch patterns were found in various studies in the literature.[34,35] Increased whorl pattern, found in our study, although without statistical significance, was also found in previous studies.[25,36,37] Our results contrast with the decreased loop, whorl and arch patterns found in some previous studies.[25,33,37] In this study, in pemphigus vulgaris patients, loop pattern was found in 50% patients, followed by whorl in 40% and arch in 10% patients, without any statistically significant difference regarding any of the dermatoglyphic patterns between pemphigus vulgaris patients and controls. To the best of our knowledge, no previous study has been conducted about the association of dermatoglyphic patterns in pemphigus vulgaris. Conclusion
Our study found some statistically significant associations between various dermatoses and specific dermatoglyphic patterns, especially the significant difference between psoriasis patients and controls regarding loop, arch and composite patterns, but no significant difference with respect to whorl pattern. Similarly, there was a statistically significant difference between alopecia areata patients and controls with respect to loop and arch patterns, but no significant difference regarding whorl pattern. There was, however, no statistically significant difference regarding any of the dermatoglyphic patterns between vitiligo and pemphigus vulgaris patients and that in controls. It is therefore suggested that the subject of dermatoglyphic patterns in various dermatoses be revisited and large scale studies be conducted in order to look for any real association between specific dermatoglyphic patterns and various dermatoses, so that high risk groups are detected and diseases diagnosed earlier. References
1. Cummins H, Midlo C. Finger prints palms and soles. An introduction to dermatoglyphics, first ed. Dover Publications, New York. 1961. pp 272.
2. Mulvihill JJ, Smith DW. The genesis of dermatoglyphics. J Pediatr 1969; 75: 579-89.
3. Lacroix B, Wolff-Quenot MJ, Haffen K. Early human hand morphology: an estimation of fetal age. Early Hum Dev 1984; 9: 127-36.
4. Babler JW. Embryonic development of epidermal ridges and their configurations. In: Platto CC, Garutto RM, Schaumann B, editors. Dermatoglyphics: Science in Transition, Birth Defects, New York: 1991; 2: 95-112.
5. Danuta ZL. Genetics of dermatoglyphic patterns. In: Quantative dermatoglyphics classification, genetics and pathology, Oxford monograph of medical genetics. New York. 1983; 10: 139-331.
6. Cummins H, Midlo C. Dermatoglyphics stigmata in mongolism. Anat Record 1936; 64: 11.
7. Penrose LS. Finger prints, palms and chromosomes. Nature 1963; 197: 933-8.
8. Stough TR, Seely JR. Dermatoglyphics in medicine. Clin Pediatr 1969; 8: 32-41.
9. Rajangam S, Janakiram S, Thomas IM. Dermatoglyphics in Down's syndrome. J Indian Med Assoc 1995; 93: 10-13.
10. Verbov JL. Dermatoglyphs in leukaemia. JMed Genet 1970; 7: 125-31.
11. Ziegler AG, Mathies R, Ziegelmayer G, Baumgartl HJ, Rodewald A, Chopra V et al. Dermatoglyphics in type-1 diabetes-mellitus. Diabet Med 1993; 10: 720-4.
12. Purvis-Smith SG. Dermatoglyphics in adults with congenital rubella. Lancet 1968; 2: 141-3.
13. Pulliam TJ, Schuster MM. Congenital markers for chronic intestinal obstruction. Am J Gastroenterol 1995; 90: 922-6.
14. Novak-Laus K, Milicić
J, Tedeschi-Reiner E, Iveković R, Korsić J, Zrinsćak O, et al. Analysis of the qualitative dermatoglyphicsof the digito-palmar complex in patients with primary open angle glaucoma. Coll Antropol. 2006; 30: 163-70.
15.
Supe S, Milicić J, Pavićević R. Analysis of the quantitative dermatoglyphics of the digito-palmar complex in patients with multiple sclerosis. Coll Antropol. 1997; 21: 319-25.
16. Weinreb HJ. Dermatoglyphic patterns in Alzheimer's disease. J Neurogenet. 1986; 3: 233-46.
17. Bejerano M, Yakovenko K, Katznelson MB, Kobyliansky E. Relationship between genetic anomalies of different levels and deviations in dermatoglyphic traits. Part 7: Dermatoglyphic peculiarities of females with cervical and endometrial carcinoma. Z Morphol Anthropol. 2001; 83: 75-108.
18. David TJ, Ajdukiewicz AB. Palmar dermatoglyphs in Wilson's disease. Br Med J 1972; 3: 825-26.
19.
Polovina S, Cvjeticanin M, MilicićJ, ProloscićTP. Dermatoglyphs and brachial
plexus palsy. Coll Antropol 2006; 30: 559-63.
20. Hale AR, Philips JH, Burch GE. Features of palmar dermatoglyphics in congenital heart disease: A report on the variants frequently associated with congenital lesions of the heart. JAMA 1961; 176: 41-45.
21.
Jelovac N, Milicić J, Milas M, Dodig G, Turek S, Ugrenović Z. Dermatoglyphic
analysis in borderline personality disorder and schizophrenia: Results of a
Croatian study. Coll Antropol 1998; 22: 141-48.
22.
Milicić J, Bujas Petković Z, Bozikov J. Dermatoglyphs of digito-palmar
complex in autistic disorder: family analysis. Croat Med J 2003; 44: 469-76.
23. Pour-Jafari H, Farhud DD, Yazdani A, Hashemzadeh Chaleshtori M. Dermatoglyphics in patients with eczema, psoriasis and alopecia areata. Skin Res Technol 2003; 9: 240-44.
24. Iqbal S, Premalatha S, Zahra A. Dermatoglyphics in vitiligo. Int J Dermatol 1985; 24: 510-13.
25. Kapur RT, Verma DR. Study of Dermatoglyphics in Dermatoses. Indian J Dermatol Venereol Leprol 1982; 48: 193-7.
26. Kumar P, Gupta A. Dermatoglyphic patterns in psoriasis, vitiligo and alopecia areata. Indian J Dermatol Venereol Leprol 2010; 76: 185-6.
27. Premalatha S. Dermatoglyphics in Darier's Disease. Indian J Dermatol Venereol Leprol 1983; 49: 122-6.
28. Passeron T, Ortonne JP. Physiopathology and genetics of vitiligo. J Autoimmun 2005; 25: 63-68.
29. Kar S, Krishnan A, Bhakta A, Dongre A. Digito-palmar dermatoglyphics in vitiligo - A case control study. J Saudi Society Dermatology Dermatologic Surgery 2012;16: 61-66.
30. Singh PK, Pandey SS, Singh G. Palmar patterns in vitiligo. Indian J Dermatol 1983; 28: 91-96.
31. Sahasrabuddhe RG, Singh G, Agarwal SP. Dermatoglyphics in vitiligo. Indian J Dermatol 1975; 21: 20-22.
32. Verma KC, Jain VK. Dermatoglyphics in vitiligo. Indian J Dermatol Venereol 1981; 47: 102-104.
33. Singh PK, Pandey SS, Singh G. Dermatoglyphics in Alopecia Areata. Indian J dermatol 1985; 30: 3-7.
34. Selmanowitz VJ, Victor S, Warburton D, Orentreich N. Fingerprint Arches in Alopecia Areata. Arch Dermatol 1974; 110: 729-34.
35. Verma KC, Jain VK, Joshi RK. Dermatoglyphics in Ichthyosis and Alopecia Areata. Indian J Dermatol Venerol Leprol 1981; 47: 35.
36. Verbov JL. Dermatoglyphic and other findings in alopecia areata and psoriasis. Br J Clin Pract 1968, 22: 257-9.
37. Sharma N, Sarin RC, Prabhakar BR. Study of Dermatoglyphics in Dermatosis.Ind J of Dermatol, Venerol and Leprol 1977; 43: 262-5.© 2014 Egyptian Dermatology Online Journal |
