|
|
Abstract
Background: Skin is the most visible organ which determines to
a great extent our appearance and plays a major function in social communication
and sexual attractiveness. Thus, the skin condition may have a considerable
impact on the patient's well being. Regardless of the psychiatric morbidity,
skin diseases can greatly affect the patient's quality of life (QOL). Thus,
patient oriented QOL measures are particularly beneficial in chronic diseases
as they assess how the diseases affect a person socially, psychologically
and physically.
Objectives: The aim of this work was to determine the impact of
some chronic dermatoses (acne vulgaris, psoriasis (Ps) and vitiligo) on
QOL among the patients in the Delta region.
Patients and Methods: The current study comprised 120 patients
who were classified into three groups; each group contained 40 patients,
(group I acne vulgaris), (group II Ps) and (group III vitiligo). All these
patients were subjected to: combined dermatological and psychological questionnaires
to assess the QOL.
Results: (Group I): As regard Cardiff Acne Disability Index
(CADI) score; the social relationships and psychological states problems
showed statistically significant difference compared with the subjective
assessment of the current acne severity. (Group II): As regard
Psoriasis Disability Index (PDI) score; the psychological, daily activities
and social relationships problems showed statistically significant difference
compared with physical and work or school problems. (Group III):
As regard Vitiligo Disability Index (VDI) score; the daily activities and
social relationships problems showed statistically significant difference
compared with feeling and symptoms, personal relationships and financial
problems. In the current study, we found that the acne vulgaris as a disease
has the worst QOL .
Conclusion: The dermatologists should understand the profound
effect of these diseases on the QOL and should know the psychosocial and
psychiatric consequences of the diseases.
Introduction
Acne vulgaris is the most common dermatological condition encountered
in adolescents. It is a chronic inflammatory disorder of pilosebaceous unit
. It commonly affects young people during the time when they are undergoing
maximum social, physical and psychological changes. [1].
Acne is neither a life-threatening nor systemic disease, yet its associated
morbidity can be devastating. [2,3].
It is typically present on facial skin, which is ready apparent to others[4].
Patients with acne frequently suffer from anxiety, depression, anger, problems
in self confidence and family relationships[5,6]
so acne have a great effect on the QOL of acne patients.
Psoriasis (Ps) is one of the most prevalent autoimmune skin diseases.
Although the initial cause of Ps remains unclear, both environmental triggers
and genetic predisposition play essential roles in the development of Ps.
[7] In Ps, there are major psychological
effects [8,9],
and the stress associated with Ps seems to be related to the way in which
the sufferer anticipates that others will react to their disease. [10]
Severe Ps affects the ability of individuals to work or study; it affects
sporting activities, especially where the skin is visible, as well as personal
and sexual relationships [11],[12].
Vitiligo is usually not harmful medically, its emotional and psychological
effects can be devastating. Regardless of a person's race and culture, white
patches of vitiligo can affect emotional and psychological well-being and
self-esteem, particularly if the condition develops on visible areas of
the body[13]. Some people who have vitiligo
feel embarrassed, ashamed, depressed, or worried about how others will react[14],[15].
A combined dermatological and psychological questionnaires will be used
to assess the effect of acne, vitiligo, Ps on the QOL by focusing on aspects
of functioning that are most affected by the disease and tend to be of greatest
importance to patients
Aim of this work
The aim of this work was to determine the impact of some chronic dermatoses
on quality of life among the patients in the Delta region.
Patients and Methods
Patients:
The current study comprised 120 patients who were selected from the Outpatients'
Clinic of Dermatology and Venereology Department, Tanta University Hospitals
from January 2011 to January 2012 after obtaining the approval of Research
Ethics Committee of the hospital (code No:670/05/12) and informed written
consent was obtained from each participant. The patients were classified
into three groups; each group included 40 patients of different clinical
varieties of acne vulgaris, Ps and vitiligo.
Inclusion criteria:
Both males and females and all age groups were included in this study,
except in acne vulgaris group (middle adolescence, from age 14 to 16 years
and late adolescence, from age 17 to 21 years old). Children were cooperative
or with cooperation of their parents.
Exclusion criteria:
Patients who refused to sign the informed consent, any associated other
skin or systemic diseases or history of psychiatric disorder, convulsion
or head trauma.
Methods:
All the patients were subjected to complete history taking including
age, gender, family history and occupation, thorough general examination
and detailed dermatologic examination.
• Every patient was subjected to clinical score to evaluate the
severity of the disease.
Group I :Acne severity in patients of the present study
was classified as mild, moderate, or severe according to Hayashi grading,
in 2008.[16]
Group II :Ps patients were classified as mild, moderate,
or severe with the Ps area and severity index (PASI).[17],
[18]
Group III :Vitiligo is classified as mild, moderate, or
severe according to vitiligo area severity index (VASI). [19]
• All the patients were subjected to combined dermatological and
psychological questionnaires to assess the QOL
Cardiff acne disability index: [20]
The patients in group I were subjected to the CADI which is a five-question
scale designed to assess the disability caused by acne-question one or two
address the psychological and social consequences of acne in general, question
three targets to those with acne of the chest or back, question four enquires
into the patient's psychological states and question five asks for patient's
(subjective) assessment of current acne severity. The response to each question
is scored from 1 to 4, the higher the score is, the greater the disability.
(Table 1)
| |
Response |
|
1.Did you feel aggressive or depressed because of your acne
vulgaris? |
Very much/ A lot/ A little/ Not at all. |
|
2.Did you think that your acne interfere with your social life
or your relationships with the other sex? |
Very much/ A lot/ A little/ Not at all. |
|
3. Did you avoid communal bathing or wearing swimming clothes
because of your acne? |
All the time/ Most of the time/ Other while/
Not at all. |
|
4.How do feel about your affected skin? |
Very depressed/ Usually interested/ Interested other while /
I don't care. |
|
5. Please, what do you think about your acne? |
The worst thing/ The main problem / Simple problem / Not a problem. |
Table
1: Cardiff acne disability index
Psoriasis disability index: [11]
The patients in group II were subjected to Ps disability index (PDI)
designed by Finaly and Coles., 1995 [11],
it is validated questionnaire covering six dimensions (symptoms and feelings,
daily activities, leisure, work and school, personal relationships and treatment)
that assess the overall impact of skin disorders and current treatments
on the patient's functioning and well being. Each question has four possible
responses, with lower scores representing a better QOL.
The PDI questionnaire was designed for use in adults, or with cooperation
of parents in case of children. It is self-explanatory and can be handed
over to the patient who is asked to fill it in without the need for a detailed
explanation. It is usually completed in 3 or 4 min. The PDI is calculated
by adding the score of each of the 15 questions, resulting in a maximum
of 60 and a minimum of zero. The higher the score, the more the QOL is impaired.
(Table 2)
|
Questions |
Response |
|
Symptoms and feelings |
|
1.How much has your Ps interfered with your carrying out work
around the house or garden? |
Very much/ A lot/ A little/ Not at all. |
|
2.How often have you worn different types or colors of clothes
because of your Ps? |
Very much/ A lot/ A little/ Not at all. |
|
3.How much more have you had to change or wash your clothes? |
Very much/ A lot/ A little/ Not at all |
|
4. How much of a problem has your Ps been at the hairdressers? |
Very much/ A lot/ A little/ Not at all |
|
5.How much has your Ps resulted in you having to take more baths
than usual? |
Very much/ A lot/ A little/ Not at all |
|
6.How much has your Ps resulted in you having to take more baths
than usual? |
Very much/ A lot/ A little/ Not at all |
|
Work or school if appropriate |
|
1.How much has your Ps made you lose time off work or school
? |
Very much/ A lot/ A little/ Not at all |
|
2.How much has your Ps prevented you from doing things at work
or school? |
Very much/ A lot/ A little/ Not at all |
3.Has your career been affected by your Ps?
e.g. promotion refused, lost a job, asked to change a
job |
Very much/ A lot/ A little/ Not at all |
|
If not at work or school |
|
1.How much has your Ps stopped you carrying out your normal
daily activities over the last four weeks? |
Very much/ A lot/ A little/ Not at all |
|
2.How much has your Ps altered the way in which you carry out
your normal daily activities over the last four weeks? |
Very much/ A lot/ A little/ Not at all |
|
Personal relationships |
|
1.Has your Ps resulted in sexual difficulties? |
Very much/ A lot/ A little/ Not at all |
|
2. Has your Ps created problems with your partner or any of
your close friends or relatives? |
Very much/ A lot/ A little/ Not at all |
|
3.How much has your Ps stopped you going out socially or to
any special functions? |
Very much/ A lot/ A little/ Not at all |
|
4.Is your Ps making it difficult for you to do any sport? |
Very much/ A lot/ A little/ Not at all |
|
5.Have you been unable to use, criticized or stopped from using
communal bathing or changing facilities? |
Very much/ A lot/ A little/ Not at all |
|
6.Has your Ps increase your smoking or drinking alcohol more
than you would do normally? |
Very much/ A lot/ A little/ Not at all |
|
7.To what extent has your Ps or treatment made your home messy
or untidy? |
Very much/ A lot/ A little/ Not at all |
Table 2:Psoriasis disability index
Vitiligo disability index: [21]
The patients in group III were subjected to Vitiligo disability index
(VDI) developed under supervision of the authors .The questions were classified
to 6 heading items: symptoms and feelings (question 1 and 2), daily activities
(question 3 and 4), leisure (question 5 and 6), personal relationships (question
7 and 8), and treatment (question 9). Each question has four possible responses,
with lower scores representing better QOL. The VDI questionnaire was designed
for use in adults, or with cooperation of parents in case of children. It
is self-explanatory and can be handed over to the patient who is asked to
fill it in without the need for a detailed explanation. It is usually completed
in 3 or 4 minutes. The VDI calculated by adding the score of each of the
9 questions, resulting in a maximum of 36 and a minimum of zero. The higher
the score, the more the QOL is impaired. (Table 3)
|
1.Did you feel aggressive or depressed because of your vitiligo? |
Very much/ A lot/ A little/ Not at all. |
|
2.How do you feel about your affected skin? |
Very depressed/ Usually interested/ Interested other while /I don't
care. |
|
3. How much your vitiligo prevented you from work or school? |
Very much/ A lot/ A little/ Not at all. |
|
4.How much has your vitiligo stopped you carrying out your normal
daily activities? |
Very much/ A lot/ A little/ Not at all. |
|
5.How much has your vitiligo stopped you going out socially or to
do any special functions? |
Very much/ A lot/ A little/ Not at all. |
|
6. Is your vitiligo making it difficult for you to do any sports? |
Very much/ A lot/ A little/ Not at all. |
|
7. Has your vitiligo resulted in sexual difficulties or difficulty
in engagement? |
Very much/ A lot/ A little/ Not at all. |
|
8.Has your vitiligo created problems with your partner or any of
your closed people? |
Very much/ A lot/ A little/ Not at all. |
|
9.How many your cessions of the disease and its psychological affects? |
Very much/ A lot/ A little/ Not at all. |
Table 3:Vitiligo disability index
As we live in Egypt and most of the patients don't know any other language
except Arabic so that we use the Arabic translation of all Questionnaires
under supervision of the authors.
Statistical analysis:
All data obtained were transferred to the statistical package for the
social sciences version 15 (IBM Co., New York, USA) for analysis. Data were
summarized using mean , standard deviation (mean± SD) using student's -t
test .Comparison between groups were made by using X2 - test and Fisher
exact test for quantitative variables Statistical significance was determined
at a level of p
≤
0.05 and highly significance at a level of p
≤ 0.001.
Results
Results of acne vulgaris patients (Group I):
The studied acne vulgaris patients included 14(35%) males and 26 (65%)
females. Their ages ranged from 16 to 35 years with a mean ±SD of (20.55±4.11)
years . As regard severity the acne vulgaris patients according to Hayashi
grading, included 10 (25%) mild cases, 18 (45%) moderate cases and 12 (30%)
severe cases with statistically non significant difference between acne
vulgaris patients. As regard QOL total score the acne vulgaris patients
included 8(20%) good QOL, 16 (40%) average QOL and 16 (40%) poor QOL with
statistically non significant difference between acne vulgaris patients
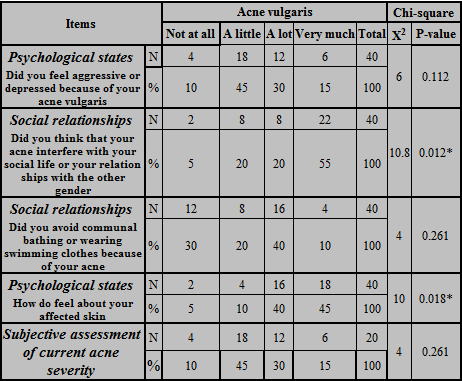
(Table 4). As regard CADI score; the social relationships and psychological
states problems showed statistically significant difference (p<0.012, 0.018
respectively) compared with subjective assessment of current acne severity
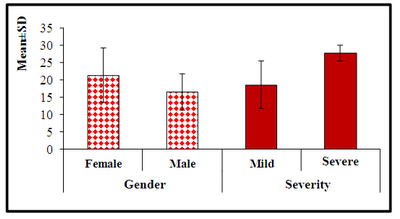
(Table 5). Regarding the relationship between CADI score and gender
in acne vulgaris group; the female patients ranged from 10.0 to 19.0 with
a mean ±SD of (14.769±2.682), the male patients ranged from 6.0 to 12.0
with a mean ±SD of (9.571±2.225) with statistically highly significant difference
(p<0.001) (Figure 1). Regarding the relationship between CADI score
and severity of acne vulgaris group; the mild cases ranged from 8.00 to
14.00 with a mean ±SD of (11.200±2.775), the moderate cases ranged from
9.00 to 18.00 with a mean ± SD of (11.444 ±2.963) and severe cases ranged
from 6.00 to19.00 with a mean ± SD of (14.167±4.446) with statistically
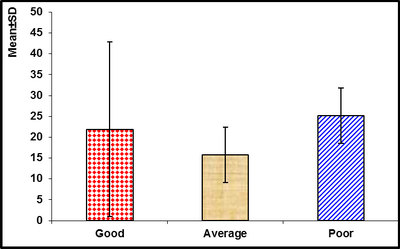
highly significant difference (p<0.001) (Figure 1). Regarding the
relationship between CADI score and age in acne vulgaris group; the good
QOL patients ranged from 22.0 to 24.0 with a mean ±SD of (22.750±0.957),
average QOL patients ranged from 16.0 to 35.0 with a mean ± SD of (20.250±6.135)
and poor QOL ranged from 17.00 to 23.00 with a mean ± SD of (19.500± 1.927).
There was no statistically significant difference (Figure 2).
|
Acne vulgaris |
N |
% |
Chi-square |
|
X2 |
P-value |
|
Gender |
Female |
26 |
65 |
1.8 |
0.18 |
|
Male |
14 |
35 |
|
Age/years |
Range |
16-35 |
|
|
Mean ± SD |
20.45±4.11 |
|
Severity |
Mild |
10 |
25 |
1.3 |
0.522 |
|
(Hayashi score) |
Moderate |
18 |
45 |
| |
Severe |
12 |
30 |
|
QOL |
Good |
8 |
20 |
1.6 |
0.449 |
|
total score |
Average |
16 |
40 |
| |
Poor |
16 |
40 |
Table 4: Distribution of acne vulgaris patients according
to gender, age, severity and quality of life total score.
*P
significant ≤ 0.05
Table 5: Specific response of Cardiff acne disability index.
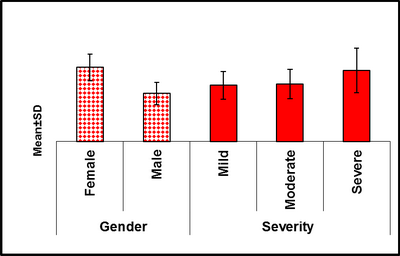
| Fig 1: Relation between Cardiff acne disability
index score with gender and severity [P-value<0.001*
and <0.001* respectively] |
|
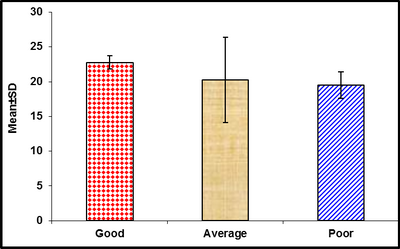
| Fig 2: Relation between Cardiff acne disability
index score and age [P-value 0.451] |
|
Results of psoriasis patients (Group II):
The studied Ps patients included 12(30%) males and 28(70%) females. Their
age ranged from 12 to 57 years with a mean ± SD of (30.50 ±11.36) years
. As regard severity the Ps patients according to PASI score; included 8
(20%) mild cases, 22 (55%) moderate cases and 10 (25%) severe cases with
statistically non significant difference between Ps patients . As regard
QOL total score; the Ps patients included 6 (15%) good QOL, 28 (70%) average
QOL and 6 (15%) poor QOL with statistically significant difference between
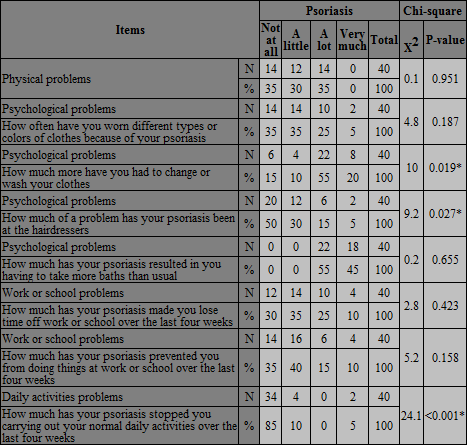
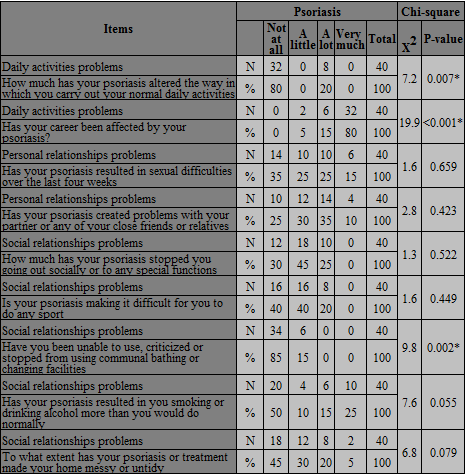
Ps patients (p<0.002) (Table 6).As regard PDI score; the psychological,
daily activities and social relationships problems showed statistically
significant difference compared with physical and work or school problems
(p<0.019, 0.027, 0.001, 0.007 respectively) (Table 7). Regarding
the relationship between PDI score and gender in Ps group; the female patients
ranged from 27.0 to 53.0 with a mean ± SD of (35.500 ± 6.970), the male
patients ranged from 32.0 to 43.0 with a mean ± SD of (37.000 ± 3.795) with
statistically non significant difference (Figure 3). Regarding the
relationship between PDI score and severity of Ps group; the mild case ranged
from 28.00 to 40.00 with a mean ± SD of (30.750±2.315), the moderate case
ranged from 27.0 to 39.00 with a mean ± SD of (31.727±4.052) and severe
case ranged from 32.0 to 53.0 with a mean ±SD of (41.00±8.396) with statistically
highly significant difference (p<0.001) (Figure 3) . Regarding the
relationship between PDI score and age in Ps group; the good QOL patients
ranged from 21.0 to 57.0 with a mean ± SD of (35.333±19.088), average QOL
patients ranged from 15.0 to 48.0 with a mean ± SD of (29.786±9.862) and
poor QOL ranged from 12.0 to 37.0 with a mean ± SD of (27.00±13.229) with
statistically no significant difference ( P-value 0.672) (Figure 4).
|
Psoriasis |
N |
% |
Chi-square |
|
X2 |
P-value |
|
Gender |
Female |
28 |
70 |
4.3 |
0.116 |
|
Male |
12 |
30 |
|
Age/ years |
Range |
21155 |
|
|
Mean ± SD |
30.20±11.36 |
|
Severity(PASI score) |
Mild |
8 |
20 |
3.2 |
0.074 |
|
Moderate |
22 |
55 |
|
Severe |
10 |
25 |
|
QOL total score |
Good |
6 |
15 |
12.1 |
0.002* |
|
Average |
28 |
70 |
|
Poor |
6 |
15 |
*P
significant< 0.005
Table 6: Distribution
of psoriasis group according to gender, age, severity and quality of life
total score.
*P significant≤ 0.05
P highly significant≤0.001
Table 7:Specific response to psoriasis
disability index.
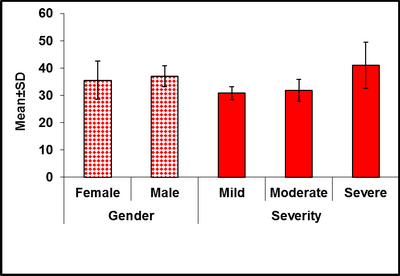
| Fig 3: Relation between psoriasis disability
index score with gender and severity [P-value 0.629
and<0.001 respectively] |
|
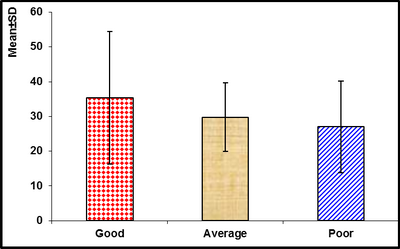
| Fig 4: Relation between psoriasis disability
index score and age [P-value 0.672] |
|
Results of vitiligo patients (Group III):
The studied vitiligo patients included 12(30%) males and 28(70%) females.
Their age ranged from 7 to 67 years with a mean ± SD of (21.65 ±15.43) years
. As regard severity the vitiligo patients according to VASI score; included
24 (60%) mild cases and 16 (40%) severe cases with non statistically significant
difference between vitiligo patients .As regard QOL total score; the vitiligo
patients included 20(50%) good QOL, 8 (20%) average QOL and 12 (30%) poor
QOL with no statistically significant difference between vitiligo patients
. As regard the site of the vitiligo; the patients were classified in to
30 (75%) patients had the disease on the exposed area and 10 (25%) patients
had the disease on the covered area with statistically significant difference
between the vitiligo patients (p< 0.002) (Table 8).As regard VDI
score; the daily activities and social relationships problems showed statistically
significant difference (p<0.001, 0.011, 0.047, 0.002 respectively) compared
with feeling and symptoms, personal relationships and financial problems.
(Table 9).Regarding the relationship between VDI score and gender
in vitiligo group; the female patients ranged from10.0 to 30.0 with a mean
± SD of (21.429±7.920); the male patients ranged from11.0 to 25.0 with a
mean ±SD of (16.500±5.244) with non statistically significant difference
(Figure 5).Regarding the relationship between VDI score and severity
of vitiligo group; the mild case ranged from 12.0 to 30.0 with a mean ±
SD of (18.67±6.92) and severe case ranged from 10.0 to 30.6 with a mean
± SD of (27.88±2.22) with statistically significant difference (p<0.038)
(Figure 5). Regarding the relationship between VDI score and age
in vitiligo group; the good QOL patients ranged from 7.00 to 67.00 with
a mean ± SD of (21.900±20.973), average QOL patients ranged from 7.00 to
23.00 with a mean ±SD of (15.750± 6.602) and poor QOL ranged from 19.00
to 34.00 with a mean ± SD of (25.167 ±6.676) with no statistically significant
difference (Figure 6). Regarding the relationship between VDI score
and the site of the disease in vitiligo group; the patients with vitiligo
in exposed area was classified to 2 (5%) good QOL, 6 (15%) average QOL and
22 (55%) poor QOL and the patients with vitiligo in covered area was classified
to 6(15%) good QOL, 2 (5%) average QOL and 2(5%) poor QOL with statistically
significant difference (p <0.028) (Figure 7).
|
Vitiligo |
N |
% |
Chi-square |
|
X2 |
P-value |
|
Gender |
Female |
28 |
70 |
6.4 |
0.011* |
|
Male |
12 |
30 |
|
Age/ years |
Range |
24654 |
|
|
Mean ± SD |
21.65±15.43 |
|
Severity |
Mild |
24 |
60 |
0.8 |
0.371 |
|
(VASI score) |
Severe |
16 |
40 |
|
QOL |
Good |
20 |
50 |
2.8 |
0.247 |
|
total score |
Average |
8 |
20 |
| |
Poor |
12 |
30 |
|
Site |
Exposed |
30 |
75 |
10 |
0.002* |
|
Covered are |
10 |
25 |
*P significant ≤ 0.05Table 8: Distribution of vitiligo group according
to gender, age, severity, quality of life total score and the site of vitiligo.
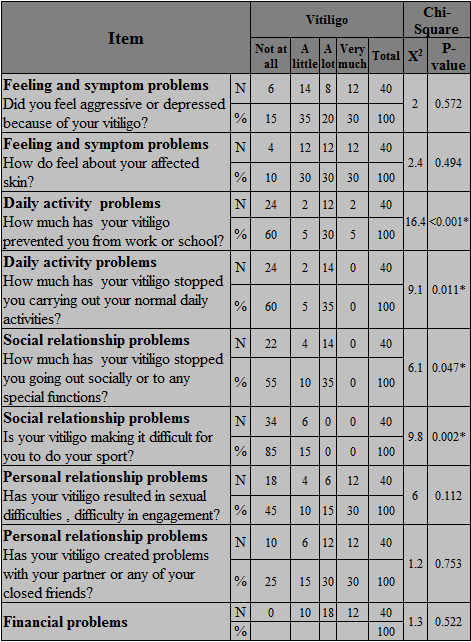
Table 9: Specific response to vitiligo disability index
| Fig 5: Relation between vitiligo disability
index score with gender and severity [P value 0.182
and 0.038 respectively] |
|
| Fig 6: Relation between vitiligo disability
index score and age [P value 0.662] |
|
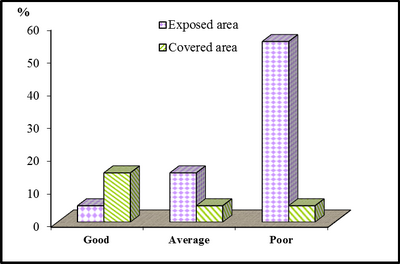
| Fig 7: Relation between vitiligo disability
index score and the site of the disease [P value 0.028] |
|
As regard the QOL total score; the acne vulgaris patients included 8(20%)
good QOL, 16 (40%) average QOL and 16 (40%) poor QOL, the Ps patients included
6 (15%) good QOL, 28 (70%) average QOL and 6 (15%) poor QOL and the vitiligo
patients included 20(50%) good QOL, 8 (20%) average QOL and 12 (30%) poor
QOL with statistically significant difference between three groups (p<0.001).
(Table 10).
Discussion
The QOL is generally measured using validated questionnaires. Several
instruments have been designed for use in many different diseases, for skin
disorders only, or for one particular disease such as acne. [22]
As regard QOL total score; the current study showed statistically non
significant difference between acne vulgaris patients, similar results was
recorded by Lauren et al., [23] . As regard
CADI score; the current study showed that, the social relationships and
psychological states problems showed statistically significant difference
compared with subjective assessment of current acne severity. These results
were in agreement with Pawin et al., [24]as
regard CADI score they reported that; relationships with friends and psychological
states problems showed statistically significant difference compared with
subjective assessment of current acne severity.
In agreement with the present study, Hanisah et al., [25]
showed that; the adolescents had particular difficulties in the areas of
emotion (felt aggressive, frustrated), social interference/difficulties
and psychological state disturbance. A study among teenage Scottish school
children reported that 50% of pupils were emotionally affected by their
acne,20 % of pupils were affected in their personal and social lives because
of their acne and 10% avoided swimming and other sports because of embarrassment.
[23]
Regarding the relationship between CADI score and gender; there was statistically
highly significant difference. In accordance with pervious studies which
found that girls generally experience more psychological morbidity than
boys; this may be due to that female patients are more concerned about their
cosmetic appearance and beauty especially at adolescent and young age. [26],
[27] On the other hand other studies showed
that; there was no significant difference in mean CADI scores between both
gender.; this may be attributed to the near equal concern about appearance
in both gender. [23], [25]
Regarding the relationship between CADI score and severity of acne vulgaris
group; the current study showed that, highly statistically significant difference
between mild, moderate and severe cases. Also, many studies were in agreement
with this finding [25,28-30],
they demonstrated strong correlation between the total score of CADI score
and acne severity; the impact on QOL increased with the facial acne severity.
On the other hand, some studies have failed to show a strong association
between acne severity and QOL. Hence, it is difficult to ascertain the extent
of disability caused by a given severity of acne, as QOL is dependent on
a host of correlating factors that are as yet poorly understood. [31,32]
Regarding the relationship between CADI score and age in acne vulgaris
group; the present study showed that, there was no statistically significant
difference. Similarly Matsuko et al.,[33]
found that no correlation between age and QOL scores. But on the other hand,
Lasek et al., [34] reported an inverse
correlation between the age of patients with acne and their QOL.
As regard QOL total score; the current study showed statistically significant
difference between Ps patients. Meanwhile, Rakhesh et al., [35]
recorded the same result.
As regard PDI score the current study showed that; the psychological,
daily activities and social relationships problems showed statistically
significant difference compared with physical and work or school problems.
A study done by Aghaei et al., [36] showed
significant relation was seen between the mean PDI score and all the scales,
except for the mean PDI and the work and school scale in females. Analysis
of the PDI questionnaire done by another study (35) and showed that; questions
related to difficulties in personal relationships and leisure activities
showed statistically significant difference compared with the questions
related to daily activities, employment and treatment-related difficulties.
Another study done by Finaly et al., [37]
showed that; the questions related to personal and social relationships
showed statistically significant difference compared with the questions
related to daily activities and treatment.
Regarding the relationship between PDI score and gender in Ps patients;
the current study showed statistically non significant difference. A study
done by Young et al., [38] was in agreement
with the present study. In contrast, another previous study has shown women
to be more likely than men to report impairment of QOL.[39]
Regarding the relationship between PDI score and severity of Ps by PASI
score; the current study showed that; statistically highly significant difference
between mild, moderate and severe cases.These findings similar to the previous
studies.[39,40]
In agreement with the current results; a study done by Rakhesh et al.,
[35] they observed highly significant correlation
of the PASI score with all subdivisions of PDI except treatment-related
activities. On the other hand, previous studies also found moderate correlation
between PASI and PDI scores.[41],[42]
At the contrary; other studies did not find any significant correlation
between PASI and PDI scores. [10], [43]
Regarding the relationship between PDI score and age; the current study
showed statistically non significant difference. On the other hand, a study
done by Saleh et al., [40] reported that
younger patients were more prone to have psychiatric morbidity and poor
QOL. These results denote that un-established social life in younger patients
makes them worry about their future resulting in more psychological distress
and psychiatric morbidity.
As regard QOL total score the current study showed no statistically significant
difference between vitiligo patients. Jalel et al., [44)]found that in their
study more than 60 % of vitiligo patients had poor QOL.
As regard VDI score, the current study showed that; the daily activities
and social relationships problems showed statistically significant difference
compared with feeling and symptoms, personal relationships and financial
problems. In agreement with the current study; a study done by Dolatshahi
et al.,[45] showed that; the daily activities
and social relationships problems showed statistically significant difference
compared with feeling and symptoms, personal relationships and financial
problems. On the other hand, previous studies reported that; feeling and
symptoms, personal relationships showed statistically significant difference
compared with the daily activities and social relationships problems. (46-
48)
Regarding the relationship between VDI score and gender in vitiligo group;
the current study showed non statistically significant difference. These
results in agreement with many studies; as they showed no statistically
significant difference in relationship between VDI score and gender. [45-50]
On the other hand, a study had done by Ongenae et al., 2004 [46]
showed women to be more likely than men to report impairment of QOL. Regarding
the relationship between VDI score and severity of vitiligo group; the current
study showed that, statistically significant difference. The current study
similar to the many previous studies. [40,45,46,47,51]
On contrast, a study done by Parsad et al., 2003[49]
showed that no statistically significant difference between VDI score and
severity of vitiligo.
Regarding the relationship between VDI score and age in vitiligo group;
the current study showed non statistically significant difference. Several
studies also reported no statistically significant difference in relationship
between VDI score and age [45,46,48,].
On contrast, other studies reported statistically significant difference
[47], [49].
Similarly, Saleh et al..[40] showed that
younger patients were more prone to have psychiatric morbidity and poor
QOL with statistically significant difference. Regarding the relationship
between VDI score and the site of the disease in vitiligo group; the current
study showed statistically significant difference between VDI and visibility
of vitiligo. In agreement with the current study; other studies found that
the vitiligo patients with visible lesions were significantly higher in
psychiatric morbidity compared to patients with non visible lesions[40],
[46]. On the other hand Dolatshahi et al.[45]
found that; no significant relation between VDI score and visibility of
the disease.
In the current study, we found that the severity of the three diseases
had significant relations to psychiatric morbidity because the disease severity
profoundly affected our patients, gave them hopeless feeling that their
skin condition will not improve especially with their bad life circumstances
and low economic support for treatment. In the current study, we found that
the acne vulgaris as a disease has the worst QOL compared with Ps and vitiligo.
The presence of acne can negatively affect QOL, self-esteem, and mood in
adolescents. Acne is associated with an increased incidence of anxiety,
depression, and suicidal ideation. The presence of these and other comorbid
psychological disorders should be considered in the treatment of acne patients
when appropriate. Successful treatment of acne with isotretinoin qualitatively
decreases depressive symptoms and improves QOL. [23]
In addition to the effect of acne on the patient, family and social relationships
may also be strained. Parents may worry about the short and long term repercussions
of their child's appearance, such as being bullied at school or having permanent
scarring from acne lesions. [52]
The study done by Saleh et al., [40]
found that; Ps had the worst QOL compared to the vitiligo as the patients'
burden from subjective symptoms such as physical disability, bleeding and
pruritus is more than vitiligo. The impact of Ps on patients' physical,
social and psychological functioning and health related QOL has been well
documented. Many patients report moderate to extreme feelings of anxiety,
anger and depression, increasing severity of Ps appears to correlate closely
with increased severity of depression and in turn, with higher frequency
of suicidal ideation. [53] On the other
hand, Jalel et al., [44] found that; vitiligo
had the worst QOL compared to Ps, atopic dermatitis and alopecia areata.
Vitiligo is an important skin disease having major impact on the QOL of
patients suffering from vitiligo. The appearance of skin can condition an
individual self-image, and any pathological alteration can have psychological
consequences. Most patients of vitiligo report feelings of embarrassment,
which can lead to a low self-esteem and social isolation.[44]
Suicidal ideation is a serious problem among sufferers of these disfiguring
dermatological diseases. In a study by Gupta et al., [54]
Ps patients had 9.7% prevalence of suicidal thoughts and 5.5% suicidal attempts,
They found that a higher disease severity in Ps was associated with a higher
prevalence of suicidal ideation. But as we live in the Islamic country and
our patients totally confident that suicidal ideation religiously unacceptable
so in our study no significant relation between dermatological disfigurement
and suicidal ideation. The QOL in our vitiligo patients was worse compared
to that of Belgian patients. This might be due to the lighter skin color
of the Belgian patients that cause less cosmetic disfigurement and the better
facilities for treatment compared to our patients. [55]
The field of dermatology can take credit for improving the quality of
patients' lives. Many skin conditions affect patients in a multidimensional
manner, ranging from emotional to social interactions, symptoms, and functional
impairment. Skin condition, which has been shown to affect QOL to an extent
similar to that seen in other chronic diseases such as cancer, arthritis,
hypertension, heart disease, diabetes, and depression.
Conclusion
Acne vulgaris, psoriasis and vitiligo are commonly associated with psychiatric
morbidity. The present study found a strong association between psychiatric
morbidity and poorer QOL in the three disease groups. It is important for
dermatologists to understand the profound effect of these diseases on the
QOL and to know the psychosocial and psychiatric consequences of these diseases.
Recommendations
Psychiatric intervention is strongly recommended, especially during the
early stages of the disease, because psychological consequences of these
dermatological diseases were found to be more common in the acute stages
of the disease. Educational programs aimed at increasing dermatologists'
awareness of mental health issues and promoting the use of psychiatric screening
questionnaires might help and increase recognition of psychiatric morbidity
in patients with skin diseases such programs are strongly recommended. Further
studies on the scope of psychopathology associated with these diseases in
order to define and hence manage the specific psychiatric diseases that
are more common in the patients. A mutual respectful collaboration between
dermatological and mental health professionals might be of help for many
patients. Dermatologists should listen carefully and with great sympathy
to their patients, complain in order to detect early psychic disturbance
that may influence the course of the disease and response to treatment.
References
1. Krowchuck DP. Managing acne in adolescent. Pediatr Clin
North Am 2000 ; 47: 841-57.
2. Hull PR , D, Arcy C . Acne, depression and suicide. Dermatol
Clin 2005 ; 23: 665-74.
3. Bowe WP, Leyden JJ, Crerand CE, et al . Body dysmorphic
disorder symptoms among patients with acne vulgaris. J Am Acad Dermatol
2007 ; 57: 222-30.
4. Fried RG , Wechsler A. Psychological problems in the
acne patient. Dermatol Ther 2006 ; 19: 237-40.
5. Koo JY . The psychological impact of acne: patient's
perception. J Am Acad Dermatol 1995; 32: 26-30.
6. Smithard A, Glazebrook C , Williams HC .Acne prevalence,
knowledge about acne and psychological morbidity in mid-adolescence: a community-based
study. Br J Dermatol 2001 ; 154: 274-9.
7. Bowcock AM , Kruger JG. Getting under the skin: The immunogenetics
of psoriasis. Nat Rev Immunol 2005; 5: 699-711.
8. Fried RG , Friedman S. Trivial or terrible? The psychosocial
impact of psoriasis. Int J Dermatol 1995 ; 34: 101-5.
9. Wahl A. The impact of psoriasis on psychological life
domains. Scand J Caring Sci 1997; 11:243-9.
10. Fortune DG , Main CJ. Quality of life in patients with
psoriasis. Br J Dermatol 1997; 137: 755-60.
11. Finaly AY, Coles EC The effects of severe psoraisis
on the quality of life of patients. Br J Dermatol 1995 ; 132: 236-44.
12. Feldman SR, Fleischer AB , Reboussin DM, et al. The
economic impact of psoriasis increases with psoriasis severity. J Am Acad
Dermatol 1997; 37:564-9.
13. Morgan M, McCreedy R , Simpson J . Dermatology quality
of life scales. A measure of the impact of skin diseases. Br J Dermatol
1998 ; 136:202-6.
14. Anderson RT , Rajagopalan R. Development and validation
of a quality of life instrument for cutaneous diseases. J Am Acad Dermatol
1999 ; 37:41-50.
15. Book O, Schmid-Ott G , Malewski P. Quality of life
patients with facial laceration. Arch Dermatol 2006 ; 297: 433-8.
16. Hayashi N, Akamatsu H , Kawashima M .Establishment
of grading criteria for acne severity. J Dermatol 2008; 35:255-60.
17. Fredriksson T , Pettersson U. Severe psoriasis- oral
therapy with a new retinoid. Dermatology 1978; 157: 238-44.
18. Langley RGB, Krueger GG , Griffiths CEM . Psoriasis:
epidemiology, clinical features, and quality of life. Ann Rheum Dis 2004
; 64: 18- 23.
19. Hamzavi I, Jain H, McLean D, et al. Parametric modeling
of narrowband UV-B photo-therapy for vitiligo using a novel quantitative
tool: the vitiligo area scoring index. Arch Dermatol 2004:; 140: 677-83.
20. Finlay AY. Dermatology patients: what do they really
need ? Clin Exp Dermatol 2000 ; 25:444-50.
21. Kent G, Al'Abadie M. Psychologic effects of vitiligo:
A critical incident analysis. J Am Acad Dermatol 1996; 35: 895-8
22. Chren MM, Lasek RJ, Quinn LM, et al . Skindex, a quality-of-life
measure for patients with skin disease: Reliability, validity and responsiveness.
J Invest Dermatol 1996; 107:707-13.
23. Lauren K D, Jenna L O , Steven R F .Acne in Adolescents:
quality of life, self-esteem, mood, and psychological disorders. Dermatol
Online J 2011; 17 : 1.
24. Pawin H, Chivot M, Beylot C, et al. Living with acne.
A study of adolescents' personal experiences. Dermatology 2007 ; 215:308-14.
25. Hanisah A, Omar K, Shah SA. Prevalence of acne and
its impact on the quality of life in school-aged adolescents in Malaysia.
J Primary Health Care 2009 ; 1:20-5.
26. Jeong E D, Sun-Mi C, Sung-Il I, et al .Psychosocial
aspects of acne vulgaris: a community-based study with Korean adolescents.
Ann Dermatol 2009 ; 21: 125-9.
27. Cotterill JA ,Cunliffe WJ. Suicide in dermatological
patients.Br J Dermatol 1997; 137:246-50.
28. Akyazı
H, Baltacı
D, Alpay K ,et al. Quality of life in adult patients with acne vulgaris
before and after treatment. Dicle Med J 2011 ; 38: 282-8.
29. Walker N , Lewis-Jones MS .Quality of life and acne
in Scottish adolescent schoolchildren: use of the children's dermatology
life quality index (CDLQI) and the Cardiff acne disability index (CADI).
J Eur Acad Dermatol Venereol 2006 ; 20: 45-50.
30. Fehnel SE, McLeod LD, Brandman J, et al. Responsiveness
of the acne-specific quality of life questionnaire (Acne-QOL) to treatment
for acne vulgaris in placebo-controlled clinical trials. Qual Life Res 2002
; 11: 809-16.
31. Yazici K, Baz K, Yazici AE, et al. Disease-specific
quality of life is associated with anxiety and depression in patients with
acne. J Eur Acad Dermatol Venereol 2004; 18: 435-9.
32. Ilgen E , Derya A .There is no correlation between
acne severity and AQOLS/DLQI scores. J Dermatol 2005 ; 32: 705-10.
33. Matsuoka Y, Yoneda K, Sadahira C, et al. Effects of
skin care and makeup under instructions from dermatologists on the quality
of life of female patients with acne vulgaris. J Dermatol 2006 ; 33:745-52.
34. Lasek RJ, Chren MM. Acne vulgaris and the quality of
life of adult dermatology patients. Arch Dermatol 1998; 134:454-8.
35. Rakhesh S V, Mariette D , Ajith S. Quality of life
in psoriasis: a study from south India. Indian J Dermatol 2008 ; 47: 600-6.
36. Aghaei S, Moradi A, Ardekani GS. Impact of psoriasis
on quality of life in Iran. IJ DVL 2009; 57: 220.
37. Finlay AY . Quality of life measurement in dermatology:
A practical guide. Br J Dermatol 1997 ; 136:305-14.
38. Young W L, Eun J Pa, Kwang H K, et al. Impact of psoriasis
on quality of life: relationship between clinical response to therapy and
change in health-related quality of life. Ann Dermatol 2010; 22: 389-96.
39. Zachariae R, Zachariae H, Blomqvist K, et al. Quality
of life in 6497 Nordic patients with psoriasis. Br J Dermatol 2004 ; 146:
1006-16.
40. Saleh HM, Samar,Salem SAM, El-Sheshetawy RS. Comparative
study of psychiatric morbidity and quality of life in psoriasis, vitiligo
and alopecia areata. Egy Dermatol Online J 2008; 4: 2.
41. Gelfand JM, Feldman SR, Stern RS, et al. Determinants
of quality of life in patients with psoriasis: a study from the US population.
J Am Acad Dermatol 2004; 51:704-8.
42. Ashcroft DM, Li Wan PA, Williams HC et al. Quality
of life measures in psoriasis: a critical appraisal of their quality. J
Clin Pharm Ther 1998 ; 23:391-8.
43. Yang Y, Koh D, Khoo L, et al. The psoriasis disability
index in Chinese patients: contribution of clinical and psychological variables.
Int J Dermatol 2005 ; 44:925-9.
44. Jalel A, Soumaya GS, Hamdaoui MH. Dermatology life
quality index scores in vitiligo: reliability and validity of the Tunisian
version. Indian J Dermatol 2009; 45: 330-3.
45. Dolatshahi M, Ghazi P, Feizy V, et al. Life quality
assessment among patients with vitiligo: comparison of married and single
patients in Iran. Indian J Dermatol 2008; 74: 700.
46. Ongenae K, Van Geel, N, De Schepper S , et al. Management
of vitiligo patients and attitude of dermatologists towards vitiligo. Eur
J Dermatol 2004; 14: 177-81.
47. Kent G ,Al-Abadie MSK. Factors affecting responses
on dermatology life quality index among vitiligo sufferers. Clin Exp Dermatol
1997 ; 21:330-3.
48. Aghaei S, Sodaifi M, Jafari P,et al. DLQI scores in
vitiligo: reliability and validity of the Persian version. BMC Dermatol
2004; 4:8.
49. Parsad D, Dogra S , Kanwar AJ .Quality of life in patients
with vitiligo. Health Quality Life Outcomes 2003; 1:58.
50. Alireza F, Navid B, Nader F, et al. What patients with
vitiligo believe about their condition? Int J Dermatol 2004 ; 43: 811-4.
51. Osman AM, Elkordufani Y, Abdullah MA .The psychological
impact of vitiligo in adult Sudanese patients. Afr J Psych 2009 ; 12:284-86.
52. Hassan J, Grogan S, Clark-Carter D, et al. The individual
health burden of
53. acne: appearance-related distress in male and female
adolescents and adults with back, chest and facial acne. J Health Psychol
2009; 14:1105-8.
54. Loo WJ, Diba V, Chawla M , et al. Dermatology life
quality index: influence of an illustrated version. Br J Dermatol 2003;
148:285-90.
55. Gupta MA, Gupta AK , Schork NJ. Suicidal ideation in
psoriasis, Int J Dermatol 1993 ; 32: 188- 90.
56. Ongenae K ,Van Geel N, De Schepper S ,et al. Effect
of vitiligo on self-reported health-related quality of life. Br J Dermatol
2005 ; 152: 1165- 72.
© 2014 Egyptian Dermatology Online Journal
|
