|
|
Abstract
Apocrine hidrocystomas are small, asymptomatic, benign cysts commonly
found in face. These tumors when in the region of the eyelids can cause
significant functional and cosmetic morbidity despite their benign nature.
Various modalities of treatment for such lesions have been enumerated in
the literature. Here, we are describing a case of giant solitary recurrent
apocrine hidrocystoma which is being managed by en-bloc excision with reconstruction
of lower eyelid.
Introduction
Apocrine hidrocystomas are benign cysts that originate from the apocrine
secretory glands of Moll. They are commonly located in head and neck region.[1]
They can be eccrine or apocrine in origin with varying diameters.Tumours
more than 20 mm are called giant apocrine hidrocystomas.[2]
To the best of our knowledge only six case reports exist that describe giant
hidrocystomas occurring on the face.[1,3,4,5]
Laktaoui et al. has reported large apocrine cyst on the eyelid measuring
20mm.[4] We present a case of giant solitary
recurrent apocrine hidrocystoma of 30mm in size located over right lower
eyelid causing cosmetic and functional morbidity. We emphasize the importance
and need for complete excision of such lesions either by complete cyst wall
removal or en bloc excision to lower the risk of recurrence.
Case History
A 46 year old male patient presented with swelling over the right lower
lid since two years hindering his visual field and causing unsightly lid
appearance (Figure 1). There was no history of impaired vision, diplopia,
watering of eyes or prior trauma. His past history revealed similar kind
of swelling at the same site for which he was operated twice. On examination
there is a solitary swelling of 3x2 cm occupying lateral 2/3rd of right
lower lid involving skin and conjunctiva, hard in consistency, with no skin
changes. Ocular mobility was full. Ophthalmic examination was otherwise
normal. The lesion was excised en-bloc and reconstruction of the lower eyelid
with cheek rotation flap was done under general anesthesia. The wound healed
well with satisfactory restoration of cosmetic appearance and full restoration
of his visual field (Figure 2). Histopathology section revealed multiple
cystic spaces of varying sizes with papillary projections. Occasional cysts
show columnar secretary cells with decapitation secretion and some double
layered epithelium. The features were consistent with apocrine hidrocystoma
with no evidence of malignant change (Figure 3). Sutures were removed on
tenth post operative day. The patient was followed up to 5 years and there
was no recurrence.
 | Fig 1:
Solitary swelling occupying lateral aspect of right lower eyelid |
|
 | Fig
2: Post operative photograph after en-block excision of the
swelling and reconstruction of lower lid |
|
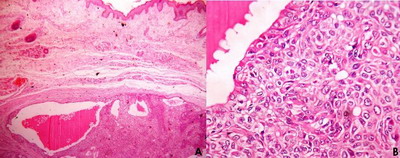 Fig
3: Histopathological section of the mass
a. low power view showing multiple cystic spaces with
decapitation secretion in the lumen (H & E,10X)
b. High power view showing cyst lined by epithelial
cells. (H & E, 40X) |
|
Discussion
Hidrocystomas, or sudoriferous cysts, are benign adnexal sweat gland
tumors. They occur as single or multiple lesions, found especially over
the eyelid but other locations like scalp, chest, palms and penis have also
been described.[1] Apocrine hidrocystomas
are characteristically asymptomatic with a diameter of 3 to 15 mm.[6]
According to the literature, out of six cases of giant apocrine hidrocystomas
that have been reported over the face, four were involving only the eyelids,[3,5]
one involved the internal canthus[4] and
one was located in intra orbital[1] region.
Ssi-Yan-Kai and Pearson have described a similar case of recurrent giant
apocrine hidrocystoma but located in the orbit.[1]
Eccrine and apocrine hidrocystomas may have similar clinical appearances.
However, the apocrine type can involve lower eyelid margins and tends to
produce oily, foamy secretions whereas eccrine type does not involve eyelid
margins and secretions are watery. Histopathologically, apocrine hidrocystomas
demonstrate multiple cystic spaces, papillary projections and an outer wall
of myoepithelial cells, in contrast to eccrine hidrocystomas which have
a single cystic cavity, no papillary projections and is lined by one or
two layers of cuboidal epithelial cells.[3]
Clinically they simulate haemangioma, epithelial inclusion cysts, lymphangiomas,
molluscum contagiosum and atypical basal cell carcinomas.[5]
Spontaneous resolution is rare and successful management is by excision
with complete cyst wall removal.[5] Medical
treatment advocated for multiple smaller lesions are laser thermo-ablation,
curettage, trichloroaceticacid, chemical ablation, and botulinum toxin whereas
surgical treatment involves complete excision of cyst wall in order to avoid
recurrence.[3]
In the present case recurrence could be due to lack of complete excision
of the cyst or failure to remove the entire capsule. We have opted for en-bloc
excision because of its recurrence and size. Surgical en- bloc excision
has been described for multiple eyelid apocrine hidrocystomas.[7]
The present case illustrates that giant ocular adnexal apocrine hidrocystoma
can cause significant functional and cosmetic disfigurement despite their
histologically benign nature.Apocrine hidrocystomas should be considered
in the differential diagnosis of eyelid mass lesions. Surgical en- bloc
excision of solitary lesion can be considered in cases of recurrent giant
apocrine hidrocystoma to reduce recurrence. In spite of our extensive literature
search in pubmed, we were unable to find similar case in Indian literature
so, the present case has been reported for its rarity and size.
References
1. Ssi-Yan-Kai IC, Pearson AR.Recurrent giant orbital apocrine
hidrocystomas. Eye 2012;26: 895-96.
2. Anzai S, Goto M, Fujiwara S, Da T. Apocrine hidrocystoma:
a case report and analysis of 167 Japanese cases. Int J Dermatol 2005;44(8):702-3.
3. Vashi N, Mandal R. Giant multi-loculated apocrine hidrocystomas.
Dermatol Online J 2010;16:16
4. Laktaoui A, Kriet M, Bouia Y, Louaya S, Zrara I, Fiqhi
A et al. Giant apocrine hydrocystoma of the internal canthus. JFr Ophtalmol
2011;34(2): 91-94
5. Sheth HG, Raina J. Giant eccrine hidrocystoma presenting
with unilateral ptosis and epiphora. IntOphthalmol 2008;28:429-31
6. Sarabi K, Khachemoune A. Hidrocystomas - a brief review.
MedGenMed 2006;8:57
7. Henderer JD,Tanenbaum M.Excision of multiple eyelid apocrine
hidrocystomas via an en-bloc lower eyelid blepharoplasty incision. OphthalmicSurgLasers
2000;31(2):157-61.© 2014 Egyptian Dermatology Online Journal
|
