|
|
Abstract
Background: Temporal triangular alopecia (TTA), also referred as congenital
triangular alopecia, is an uncommon dermatosis of unknown etiology. It is
characterized by a non-scarring, circumscribed alopecia often located unilaterally
in the fronto-temporal region that usually emerges at ages 2-9 years. Differential
diagnosis of other types of localized alopecia such as alopecia areata is
necessary in some cases.
Objective: To evaluate the potential benefit of trichoscopy in the clinical
diagnosis of TTA.
Methods: Trichoscopic examination of 15 patients suffering from TTA using
the DermLite II Pro and 10X optical zoom by Samsung S4 Zoom camera and their
dermoscopic findings were done.
Conclusion: Dermoscopy is a noninvasive tool that aids in the differential
diagnosis of TTA.
Introduction
Dermoscopy is a non-invasive diagnostic tool that allows the recognition
of morphologic structures not visible by the naked eye. Scalp dermoscopy
is very useful for the evaluation of patients with hair and scalp disorders.
The main advantage of dermoscopy in the evaluation of hair disorders is
the fact that large areas can be swiftly screened including eyebrows and
eyelashes that maybe difficult to evaluate using different methods [1].
Temporal triangular alopecia, is also known as congenital triangular
alopecia [2]; however the term congenital
triangular alopecia has become inadequate because most cases arise at ages
2-9 years and the disease may even manifest itself in the adulthood [3];
it is an uncommon form of alopecia of unknown etiology. It was first reported
by Sabouraud in 1905 [4]. According to Yamazki
and coworkers, around 74 cases have been reported till 2010 [3].
Although it usually emerges sporadically, reports of familial cases suggest
the presence of a para-dominant inheritance [5,6].
TTA commonly manifests itself as a spear-shaped, oval, round or triangular
area of alopecia unilaterally located in the fronto-temporal region [3,7],
however it may affect other areas of the scalp, including the occipital
region, and it may also be bilateral [8].
Sometimes there is a small fringe with terminal hairs at the front edge
of the lesion and even a tuft of hair at the center of the lesion was reported
in some cases [5,6].
Some diseases have been associated with TTA, such as: Down syndrome,
iris nevus syndrome, phakomatosis pigmento vascularis, congenital heart
disease, bone and tooth abnormalities, mental retardation and congenital
aplasia cutis [9]. The main differential
diagnoses are alopecia areata, trichotillomania, traction alopecia and congenital
aplasia cutis [7].
Hair implantation and surgical excision of the lesion are the main therapeutic
proposals in cases with significant aesthetic and emotional injury [10].
Bang and colleagues described the first successful case using topical minoxidil.
Nevertheless, there is no scientific evidence confirming the efficacy of
such treatment [11].
Aim of the work
This study was undertaken to evaluate the potential utility of a handheld
dermatoscope in the clinical diagnosis of TTA.
Patients & Methods
Clinical and dermoscopic examination was performed for 15patients suffering
from TTA using the DermLite II Pro (3Gen, Inc., San Juan Capistrano, California,
USA.) and 10X optical zoom by Samsung S4 Zoom camera (Samsung Electronics
Co., Ltd., Yeongtong-Gu Suwon-Shi, South Korea) and their dermoscopic findings
were reported.
Results
The dermoscopic features of the 15 patients with TTA were analyzed and
showed: (Figures 1-3)
- Vellus hairs in 15 patients (100%).
- Reduced follicular ostia in 6 patients (46.7%).
- Diffuse erythema in 5 patients (33.3%).
- Hypotrichosis in 5 patients (33.3%).
- White dots in 4 patients (26.7%).
- Central tuft of terminal hair in 1 patient (6.7%).
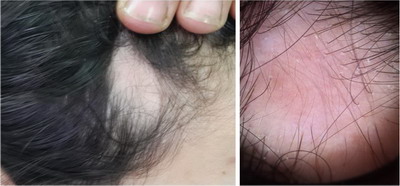 | Fig. 1:
Clinical and dermoscopic images of a patient showing only vellus
hair, diffuse erythema, diminished follicular ostia, white dots
and hypotrichosis. |
|
 | Fig.2:
Clinical and dermoscopic images of a patient showing affection
of the frontal area and dermoscopically there is only vellus
hair and hypotrichosis. |
|
 | Fig.3: Clinical and dermoscopic images of patient showing abundant vellus
hair with central tuft of terminal hair, diminished follicular ostia and
hypotrichosis. |
|
Discussion
Temporal triangular alopecia is a non-inflammatory and non-scarring form
of alopecia that remains stable throughout life [7].
Alopecia areata is the main differential diagnosis of TTA. Dermoscopy helps
to differentiate between these two diseases, avoiding the performance of biopsies
to confirm the diagnosis [6]. Dermoscopic
findings in our patients included normal follicular openings with vellus
hairs covering the area of alopecia and terminal hairs on the outskirts
of the lesion, reduced follicular ostia, diffuse erythema, hypotrichosis
and white dots. Black and/or yellow dots and 'exclamation mark' hairs, which
are present in alopecia areata, were absent in our patients so we could
confirm our diagnosis as TTA and exclude AA by simple, easy and non-invasive
tool.
In a study conducted by Inui and colleagues in 2012, the authors stressed
on the importance of the diagnostic criteria of TTA and proposed the following
criteria: I) triangular or spear-shaped area of alopecia involving the fronto-temporal
region of the scalp; II) dermoscopy reveals normal follicular openings with
vellus hairs surrounded by normal terminal hair; III) dermoscopy shows absence
of yellow and black spots, dystrophic hairs, and decreased follicular openings;
IV) persistence of no significant hair growth after dermoscopic and clinical
confirmation of the existence of vellus hairs [7],
however we report the presence of reduced number of follicular ostia as
well as the presence of white dots which may be denoting cicatrization of
those hair follicles suggesting the overall decreased number of follicles
in these patients, which is consistent with the findings of Silva and coworkers
in 2010 [12].
Conclusion
Dermoscopy is a noninvasive tool that aids in the differential diagnosis
of TTA. This method avoids invasive diagnostic procedures and ineffective
treatments.
References
1. Tosti A. Dermoscopy of hair shaft disorders. Int J Trichology
(2011); 3(Suppl1): S4.
2. 2. García-Hernández MJ, Rodríguez-PichardoA& Camacho
F. Congenital triangular alopecia (Brauer nevus)PediatrDermatol. 1995; 12:
301–3.
3. Yamazaki M, Irisawa R &Tsuboi R. Temporal triangular
alopecia and a review of 52 past cases. J Dermatol. 2010; 37: 360-2.
4. Sabouraud R. Manuel élémentaire de dermatologie topographique
régionale. Paris: Masson et cie; 1905. p. 197.
5. Assouly P & Happle R. A hairy paradox: congenital triangular
alopecia with a central hair tuft. Dermatology. 2010; 221:107-9.
6. 6. Taş B, Pilanci O & Başaran K. Congenital temporal
triangular alopecia: a typical Brauer nevus. Acta Dermatovenerol Alp
Pannonica Adriat. 2013; 22: 93-4.
7. Inui S, Nakajima T &Itami S. Temporal triangular alopecia:
trichoscopic diagnosis. J Dermatol. 2012; 39: 572-4.
8. Sarifakioglu E, Yilmaz AE, Gorpelioglu C & Orun E. Prevalence
of scalp disorders and hair loss in children. Cutis. 2012; 90: 225-9.
9. Lederer D, Wilson B, Lefesvre P, Poorten VV, Kirkham
N &Mitra D. Atypical findings in three patients with Pai syndrome and literature
review. Am J Med Genet A. 2012; 158A: 2899-904.
10. Chung J, Sim JH, Gye J, Namkoong S, Hong SP, Kim MH.
Successful hair transplantation for treatment of acquired temporal triangular
alopecia. Dermatol Surg. 2012; 38: 1404-6.
11. Bang CY, Byun JW, Kang MJ, Yang BH, Song HJ, Shin J,
et al. Successful treatment of temporal triangular alopecia with topical
minoxidil. Ann Dermatol. 2013; 25: 387-8.
12. Silva CY, Lenzy YM & Goldberg LJ. Temporal triangular
alopecia with decreased follicular density.J Cutan Pathol. 2010 May; 37(5):
597-9.© 2015 Egyptian Dermatology Online
Journal
|
