|
|
Abstract
Background: White rosettes structures seen during dermoscopic examination was thought to be specific to actinic keratosis, however this view gradually changed towards a wider one explaining that they are the result of reflection of polarized light by various keratinous structures, hence visualized in a variety of skin conditions.
Objective: Documenting the non-specificity of the dermoscopic white rosettes structures in the diagnosis of actinic keratosis.
Methods: Documentation of 12 cases with white rosette structures seen on dermoscopic examination using the DermLite II Pro and
10X optical zoom by Samsung S4 Zoom camera.
Conclusion: Dermoscopic white rosettes though most frequently seen in actinic keratosis, are non-specific in their diagnosis. Introduction
Dermoscopy, the imaging technique used to visualize structures under the skin surface, is widely considered as a valuable tool able to increase diagnostic accuracy compared with clinical evaluation [1,2]. It could be used as a rapid noninvasive tool for the diagnosis of pigmented and nonpigmented skin lesions[3]. Dermoscopy requires a high quality magnifying lens and a powerful lighting system which can be either non-polarized [NP] or a polarized light [PD] to allow examination of skin structures and patterns [4]. During the past 40 years, the development of dermoscopy implied the use of NP light and immersion fluids; therefore, figures in atlases and dermoscopy-focused papers, and the terminology that was created, were completely based on these kinds of images [1,2,5]. More recently, new dermoscopes based on polarized light emerged on the market, giving rise to a series of papers describing new features observed specifically by PD (6), as white shiny structures which including white shiny lines, white shiny areas and rosettes, and these features can only be observed under PD [7]. Patients & Methods
Twelve patients during dermoscopic examination using the DermLite II Pro (3Gen, Inc., San Juan Capistrano, California, USA.) and 10X optical zoom by Samsung S4 Zoom camera (Samsung Electronics Co., Ltd., Yeongtong-Gu Suwon-Shi, South Korea) were found to have white rosette structures, they were reported and documented. Results
Nine of the twelve patients had a well-established diagnosis of actinic keratosis
(Fig. 1), however the other three were not, two had secondary cicatricial alopecia
(Fig. 2), and the third suffered from lichen planus (Fig. 3).
 |
Fig.1 Clinical and dermoscopic images of actinic keratosis
patient showing multiple white rosettes (10 x). |
|
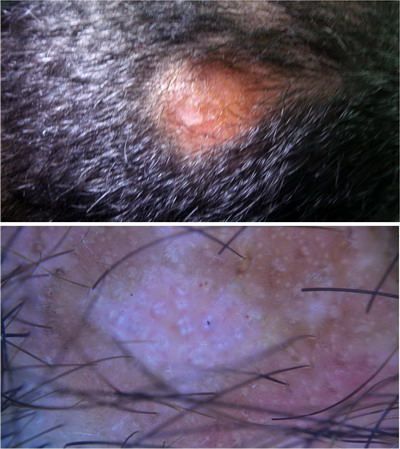 | Fig.2 Clinical and dermoscopic images of secondary cicatricial alopecia patient showing multiple white rosettes (22 x). |
|
 | Fig.3 Clinical and dermoscopic images of lichen planus patient showing single white rosette (10 x). |
|
Discussion
White rosettes are depicted as four white points arranged as four-leaf clover or as leaves radiating out from central stem. Until recently rosettes were deemed to be a significant dermoscopic structure observed only in actinic keratosis and squamous cell carcinoma and their presence was thought to support these diagnoses, however this view changed as it was documented in a range of skin lesions [8]. Rosettes vary in size from 0.2 to 0.5 mm and are believed to be attributed to an optical effect of the polarized light and its interaction with adnexal openings that are narrowed or filled with keratin, larger rosettes may be attributed to concentric perifollicular fibrosis [7]. It can be also seen in a variety of cutaneous neoplasms including: basal cell carcinoma, hypomelanotic melanoma, lichen planus like keratosis and flat seborrheic keratosis [9]. Recently white rosettes are seen in dermatofibromas, urticarial dermatitis and in cicatricial alopecia of lichen planopilaris [10,11]. In our study, we document the presence of white rosettes in other dermatoses than actinic keratosis and squamous cell carcinoma which supports the theory attributed to an optical effect of the polarized light and its interaction with adnexal openings that are narrowed or filled with keratin, and to the best of our knowledge we are the first ones to report its presence in cases of lichen planus or cicatricial alopecia. Conclusion
White rosettes are not lesion specific and can be seen in various cutaneous lesions, even in inflammatory diseases, however they are still most commonly seen in cases of actinic keratoses. References
1. Kittler H, Pehamberger H, Wolff K, Binder M. Diagnostic accuracy of dermoscopy. Lancet Oncol 2002; 3:159-163.
2. Benvenuto-Andrade C, Agero A, Dusza S, Halpern A, Marghoob A. Level of confidence in diagnosis: clinical examination versus dermoscopic examination. Dermatol Surg 2006; 32:742-748.
3. Bassoli S and Seidenari S. Benefits of polarized versus nonpolarized dermoscopy. Expert Rev Dermatol 2010; 5:17-21.
4. Oakley A: Dermoscopy. http://www.dermnetnz.org/procedures/dermoscopy.html (accessed 17 June 2015).
5. Argenziano G, Soyer HP, Chimenti S Talamini R, Corona R, Sera F, Binder M, Cerroni L et al . Dermoscopy of pigmented skin lesions: results of a consensus meeting via the internet. J Am Acad Dermatol 2003; 48:679-693.
6. Anderson RR. Polarized light examination and photography of the skin. Arch. Dermatol 1991; 127:1000-1005.
7. Liebman TN, Rabinovitz HS, Dusza SW, Marghoob AA. White shiny structures: dermoscopic features revealed under polarized light. J Eur Acad Dermatol Venereol 2012; 26: 1493-1497.
8. Cuellar F, Vilalta A, Puig S, Palou J, Salerni G, Malvehy J. New dermoscopic pattern in actinic keratosis and related conditions. Arch Dermatol 2009; 145: 732.
9. Lee JH, Won CY, Kim GM, Kim SY. Dermoscopic features of actinic keratosis and follow up with dermoscopy: a pilot study. J Dermatol 2014; 41:487-493.
10. Liebman T, Scope A, Rabinovitz H, Braun R, Marghoob A. Rosettes May Be Observed in a Range of Conditions Arch Dermatol. 2011; 147(12):1468.
11. Haspeslagh M, No€e M, De Wispelaere I, Degryse N, Vossaert K, Lanssens S, Facchetti F, Van Den Bossche K, Brochez L. Rosettes and other white shiny structures in polarized dermoscopy: histological correlate and optical explanation. J Eur Acad Dermatol Venereol. 2015; 29.© 2015 Egyptian Dermatology Online Journal |
