|
|
Abstract
The most common sarcoma in the inguinal areas is a
liposarcoma, which commonly occurs in adults. A liposarcoma is a bulky
yellow tumor similar to a lipoma but generally more complex and contains
areas of prominent sclerosis. We report a case of a 45 year old male who
reported to the department of surgery with multiple swellings of the groin
since 2 years. The histopathological examination from the masses revealed a
tumor mass composed of well-differentiated adipocytes interspersed by areas
with spindle cell proliferation. After confirmation of the diagnosis of
liposarcoma, excision was done. The case is reported because of its rarity.
Introduction
Liposarcoma is a rare tumour of the groin which is
difficult to differentiate from a lipoma. Lipoma is the most common benign
tumor of the inguinal region. The lipoma is seen as a hyperechoic mass on
sonography, which may be difficult to differentiate from a liposarcoma [1,2].
Other differential diagnosis of groin swelling includes epidermoid cyst. An
epidermoid cyst develops from a remnant of ectodermal tissues misplaced
during embryogenesis and often has a thin wall lined by stratified squamous
epithelium surrounding a mixture of desquamated debris, cholesterol,
keratin, and water. On sonography, it usually appears as a hypoechoic mass
with internal echogenicity, which can be explained by keratin materials
within the mass [3].
Other benign tumors of the groin include leiomyomas, dermoid cysts and
lymphangiomas.
Most malignant tumors in the inguinal region are
sarcomas because most of the components of the cord are derived
embryologically from mesodermal tissues. The most common sarcoma in the
inguinal areas is a liposarcoma, which commonly occurs in adults. A
liposarcoma is a bulky yellow tumor similar to a lipoma but generally more
complex and contains areas of prominent sclerosis [4].
The sonographic findings of a liposarcoma are variable and non-specific.
On the base of this case attention is called to this
rare disease. Early diagnosis and complete resection plays key role in the
treatment of liposarcoma. Liposarcoma usually occurs in the deep soft
tissues of extremities and in the retro- peritoneum. It is the most common
type of soft tissue sarcoma accounting for 30% of all mesenchymal tumors.
There are no metastases and the overall prognosis is good. Different studies
showed that the majority of dedifferentiated liposarcomas presented as de
novo lesions, whereas the remainder developed as a late complication of a
pre- existing well-differentiated liposarcoma [5,6].
Commonest sites involved by dedifferentiated liposarcoma are
retro-peritoneum, extremities, trunk, scrotum/spermatic cord, and also
subcutis.
Case Report
A 45 year old male
reported to the department of surgery with multiple swellings of the groin
since 2 years. There was no history of pain in the groin. He denied any
recent trauma to that area. Initially the swellings were smaller in size,
but gradually increased in size over a period of one year and thereafter the
size of the swellings remained constant. On local examination, four
swellings were seen in the groin area (fig.
1). The scrotum and penis were also swollen
and distorted. The swellings had a soft consistency and were freely mobile
without any fixation to the underlying structures. The physical examination
revealed no discernable loss of motor or sensory lower extremity function.
There were no specific abnormalities in the laboratory data, and the tumor
markers were within normal limits.
 | Fig 1:
Multiple swellings of the groin. |
|
The swellings were
diagnosed as multiple lipomas and histopathological examination was
performed of the groin masses. The histopathology from the masses revealed a
tumor mass composed of well-differentiated adipocytes interspersed by areas
with spindle cell proliferation (fig. 2).
In between lipoblasts were seen. The spindle cell area was mild to
moderately cellular. The cells were separated by abundant collagen
deposition and showed plump nuclei without any mitotic figures. The spindle
cells were seen infiltrating the adipose tissue, muscle fibers in the
periphery, and reaching almost up to the skin entrapping the skin adnexa. No
areas of hemorrhage or necrosis were seen.
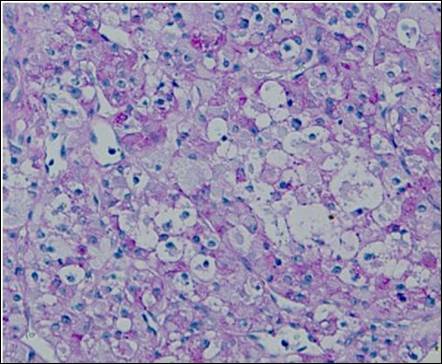 | Fig
2: H&E stained sections showing tumor mass composed of
well-differentiated adipocytes interspersed by areas with spindle
cell proliferation. |
|
The ultrasonography of the groin swellings was done
and it showed well defined hypoechoic masses with a minimal internal flow.
After the histopathological reporting which confirmed
it to be multiple liposarcomas of the groin, the excision of the groin
masses was done. Intra-operatively, the tumor was observed to roll up the
isolateral spermatic cord and testicular vessels, which led to the
differential diagnosis of liposarcoma. The tumor was then widely resected
along with the left testis, spermatic cord, and testicular vessels.
Histopathologic study confirmed the diagnosis of well-differentiated
liposarcoma, but no malignant cells were found in any of the surgical
margins. The post-operative course of the patient was uneventful. A
periodical follow-up was performed every 3 months and no evidence of
recurrence or metastasis was seen for 6 months after his operation, without
any postoperative adjuvant therapy. The case is reported because of its
rarity.
Discussion
Liposarcoma is a rare mixed histologic subtype defined
by the association of well-differentiated liposarcoma and a non-lipogenic
sarcoma of variable histological grade usually with histologically abrupt
transition [7].
According to WHO, low-grade dedifferentiated liposarcoma is defined as bland
spindle cells with a fascicular pattern with cellularity intermediate
between well-differentiated sclerosing liposarcoma and usual high-grade
areas. The behavior of dedifferentiated liposarcoma as a whole is that of a
high-grade sarcoma [8].
Good prognosis in de novo dedifferentiated liposarcomas seems unrelated to
the extent, grade, or morphologic pattern of dedifferentiation. However,
high mitotic activity in the dedifferentiated component was associated with
more aggressive clinical course [9].
The prognosis of liposarcomas with de-differentiated component of entirely
low grade was more similar to traditional liposarcoma than to that of
well-differentiated liposarcoma [10].
However, it is suggested that low-grade differentiation may represent a
precursor lesion of high-grade differentiation.
Conclusion
Liposarcoma can develop into either low-grade or high-grade
de-differentiated liposarcoma over a variable period of time. Prognosis is
unrelated to the grade or extent but is related with mitotic activity of the
dedifferentiated area. The case is rare and hence reported.
References
1. Shadbolt CL, Heinze SB, Dietrich RB. Imaging of groin masses: inguinal anatomy and pathologic conditions revisited. Radiographics 2001; 21: 261- 271.
2. Van den Berg JC, Rutten MJ, de Valois JC, Jansen JB, Rosenbusch G. Masses and pain in the groin: a review of imaging findings. Eur Radiol 1998; 8: 911- 921.
3. Henricks WH, Chu YC, Goldblum JR, Weiss SW. Dedifferentiated liposarcoma:
a clinico-pathological analysis of 155 cases with a proposal for an expanded
definition of dedifferentiation. Am J Surg Pathol 1997; 21: 271- 281.
4. McCormick D, Mentzel T, Beham A, Fletcher CD. Dedifferentiated liposarcoma. Clinicopathologic analysis of 32 cases suggesting a better prognostic subgroup among pleomorphic sarcomas. Am J Surg Pathol 1994; 18: 1213- 1223.
5. Takahira T, Oda Y, Tamiya S, Yamamoto H, Kobayashi C, Izumi T, et al. Alterations of the RB1 gene in dedifferentiated liposarcoma. Mod Pathol 2005; 18: 1461- 1470.
6. Weiss SW, Rao VK. Well-differentiated liposarcoma (atypical lipoma) of deep soft tissue of the extremities, retroperitoneum, and miscellaneous sites. A follow-up study of 92 cases with analysis of the incidence of "dedifferentiation". Am J Surg Pathol 1992; 16: 1051- 1058.
7. Singer S, Corson JM, Gonin R, Labow B, Eberlein TJ. Prognostic factors predictive of survival and local recurrence for extremity soft tissue sarcoma. Annals of Surgery. 1994; 219: 165- 173.
8. Lewis JJ, Brennan MF. Soft tissue sarcomas. In: Sabiston D, editor. The Biological Basis of Modern Surgical Practice. 15th ed. New York, NY: W. B. Saunders; 1997. pp. 528- 534.
9. Vezeridis MP, Moore R, Karakousis CP. Metastatic patterns in soft-tissue sarcomas. Archives of Surgery 1983; 118: 915- 918.
10. Brennan MF. The enigma of local recurrence. The Society of Surgical Oncology. Annals of Surgical Oncology 1997; 4: 1- 12.© 2010 Egyptian Dermatology Online Journal |
