|
|
Summary:
A 22 years old male patient complaining of
erythematous ill-defined multinodular firm mass with areas of ulceration
affecting his left thumb & the thenar eminence of 3 years duration.
Histopathological examination revealed hyperplastic epidermis with
multiple dermal nodules composed of epithelioid cells with eosinophilic
& pleomorphic cytoplasm. Immuno-histochemical studies revealed that the
cells are positive for vimentin, pancytokeratin and epithelial membrane
antigen (EMA).
Introduction:
Epithelioid sarcoma (ES) was first described by
Enzinger in 1970. It's a sarcoma simulating a granuloma or a carcinoma.
This rare malignant tumour occurs in adolescents and young adults. It is
usually located on the distal extremities (hands, fingers and forearm);
rarely occurs on the pelvis, perineum and vulva [1].
Case presentation:
A 22 years old male patient presented to the
outpatient clinic at Al-Haud Al-Marsoud Hospital, complaining of
erythematous ill-defined multinodular firm mass with areas of ulceration
affecting his left thumb and the thenar eminence of 3 years duration,
with history of recurrence after previous excision (fig.
1).

| Fig 1: Erythematous ill defined multi-nodular
firm mass with areas of ulceration affecting the left
thumb and the thenar eminence. |
|
Our clinical differential diagnoses of the case
included: atypical mycobacterial infection, lupus vulgaris, squamous
cell carcinoma, low grade malignant vascular tumor and angiosarcoma.
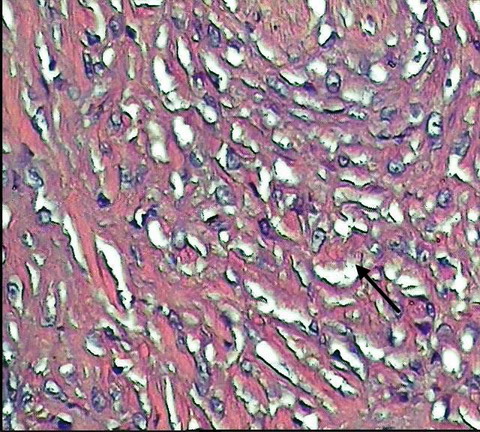
Histopathological examination revealed
hyperplastic epidermis with multiple dermal nodules composed of
epithelioid cells with eosinophilic and pleomorphic cytoplasm. The
nodules were embedded in collagenous fibrous stroma, and surrounded by
lymphocytic infiltrate with areas of haemorrhage and necrosis. Higher
power examination showed the tumour cells surrounding central zones of
necrosis (fig. 2- 6).
So according to these findings, we excluded atypical mycobacterial
infection, lupus vulgaris and squamous cell carcinoma.
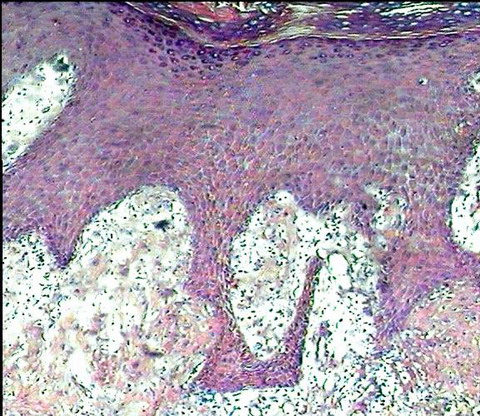
| Fig 2: H&E stained section showing hyperplastic
epidermis. |
|
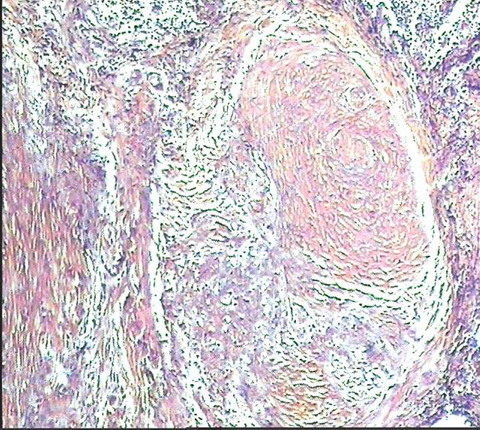
| Fig 3: H&E stained section showing multiple
dermal nodules embedded in collagenous fibrous stroma. |
|
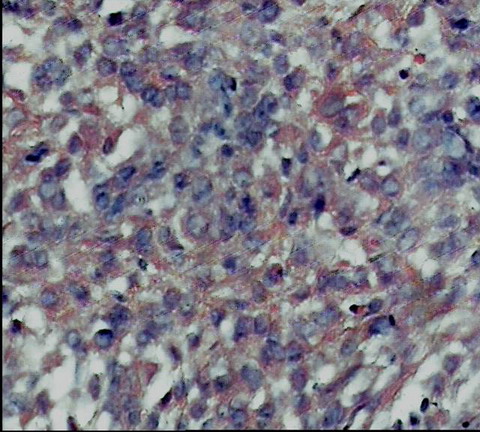
| Fig 4: The nodules are composed of epithelioid
cells with eosinophilic & pleomorphic cytoplasm. |
|
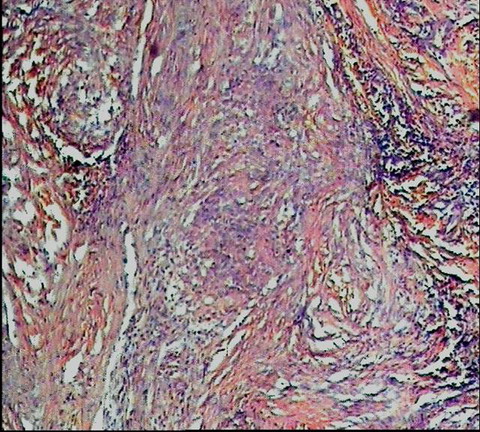
| Fig 5: Nodules are surrounded by lymphocytic
infiltrate, areas of haemorrhage and necrosis. |
|
| Fig 6: Tumor cells surrounded central zones
of necrosis. |
|
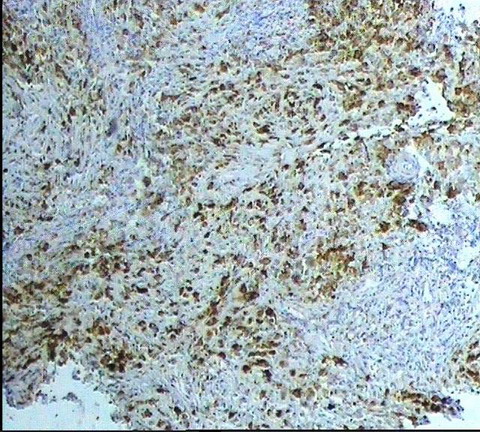
Immuno-histochemical studies were done for further
assessment of vascular origin of the tumour, but surprisingly the cells
were negative for CD 34 (fig. 7),
factor 8 (fig. 8)
and S100 protein (fig. 9),
leading us to exclude these vascular entities (low grade malignant
vascular tumor and angiosarcoma). So, we proceeded with other immune-histochemical
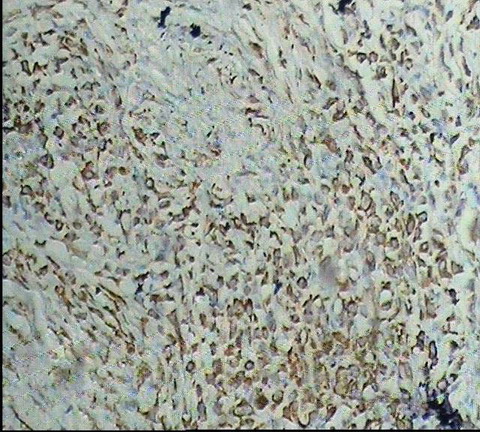
markers which revealed that the cells are positive for EMA (fig.
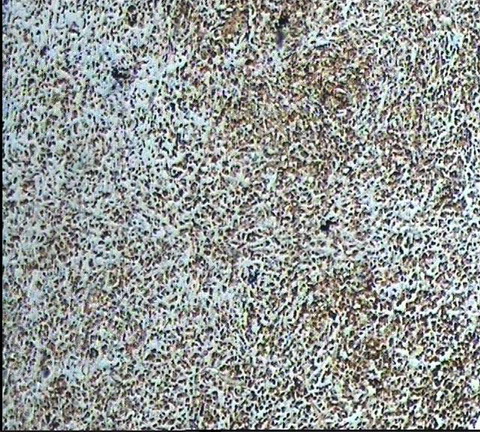
10), pancytokeratin (fig.
11) and vimentin (fig.
12), which are consistent with epithelioid
sarcoma which was our final diagnosis.
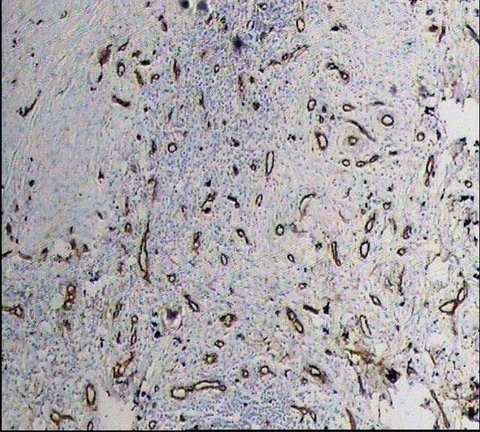
| Fig 7: CD34 was negative. |
|
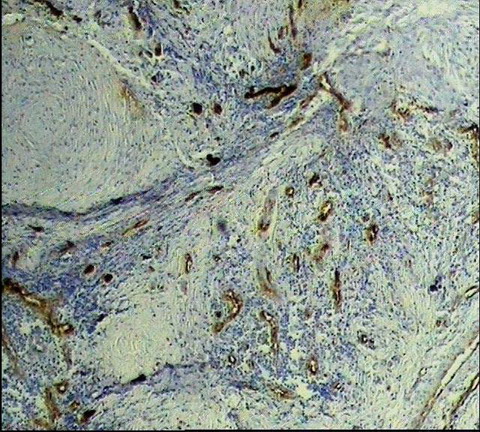
| Fig 8: Factor 8 was negative. |
|
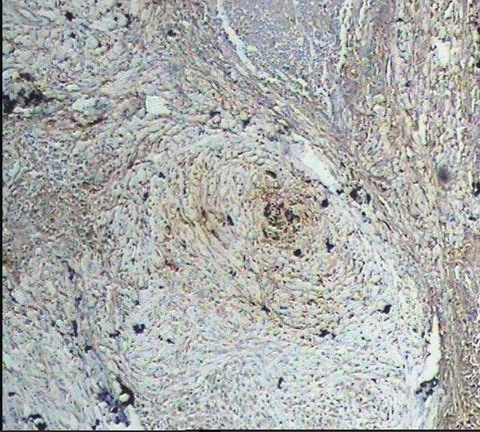
| Fig 9: S100 protein was negative. |
|
| Fig 10: EMA was positive. |
|
| Fig 11: Pan- cytokeratin was positive. |
|
| Fig 12: Vimentin was positive. |
|
Discussion:
Epithelioid sarcoma is a distinctive malignant
soft-tissue tumour composed of cells with epithelial differentiation. It
is an uncommon tumour, affecting males more often than females and
tending to begin in early adult life [1,2].
The presenting sign can be a painless slowly growing firm, dermal nodule
or lobular subcutaneous tumour that grows outwards and may ulcerate
early. These nodules surrounded by fibrous tissue and fat. The cut
surface is grayish-white and flecked or mottled with yellow or brown
spots, reflecting the presence of areas of necrosis. The distal
extremities are the usual situation for the tumour, particularly the
flexor aspect of the finger and the palm [3,4].
Microscopically the nodules are composed masses of
large, round, polygonal or spindle cells with acidophilic cytoplasm. The
larger nodules have necrotic centers and show the so-called
'geographical necrosis', which may be mistaken on scanning power
microscopy for a granuloma. Tumour cells show clear histological,
ultrastructural and immune-histochemical evidence of epithelial
differentiation. Local recurrence after excision is common and
metastasis, principally to lymph nodes, lung and pleura may occur [5,6].
Immuno-histochemically, tumour cells of ES are
positive for keratin and EMA. They also express vimentin, and in 50% of
the cases they are positive for CD34 [7].
Complete removal by surgical excision is essential
if local recurrence and eventual metastasis are to be avoided. Surgical
excision followed by radiotherapy is often recommended. Involvement of
regional lymph nodes is associated with distant metastasis and death.
The survival rate has been estimated to be between 65% and 70% [5,8].
Features associated with poorer prognosis include male sex, older age at
diagnosis, proximal location, tumour size, mitotic rate, necrosis,
vascular invasion and local recurrence and lymph node metastasis [5,6,8].
References
1. Enzinger F. Epithelioid sarcoma: a sarcoma simulating
granuloma or carcinoma. Cancer 1970; 26: 1029- 1041
2. Fletcher CDM, McKee PH. Sarcomas: a clinic-pathological
guide with particular reference to cutaneous manifestation. Clin Exp Dermatol
1984; 9: 451- 465
3. Santiago H, Feinerman LK, Lattes R. Epithelioid sarcoma:
a clinical and pathologic study of 9 cases. Hum Pathol 1972; 3: 1706- 1710
4. Evans HL, Baer SC. Epithelioid sarcoma: a clinic-pathologic
and prognostic study of 26 cases. Semin Diagn Pathol 1993; 10: 286- 291
5. Halling AC, Wollan PC, Pritchard DJ, Vlasak R, Nascimento
AG. Epithelioid sarcoma: a clinicopathologic review of 55 cases. Mayo Clin
Proc 1996; 71: 636- 642
6. Prat J, Woodruff JM, Marcove RC. Epithelioid sarcoma:
an analysis of 22 cases indicating the prognostic significance of vascular
invasion and regional lymph node metastases. Cancer 1978; 41: 1472- 1487
7. Arber DA, Kandalaft PL, Mehta P, Battifora H. Vimentin-negative
epithelioid sarcoma: the value of an immunohistochemical panel that includes
CD34. Am J Surg Pathol 1993; 17: 302- 307
8. Chase DR, Enzinger FM. Epithelioid sarcoma: diagnosis,
prognostic indicators and treatment. Am J Surg Pathol 1985; 9: 241- 263.
© 2010 Egyptian Dermatology Online Journal
|
