|
|
Summary
An 18 years old girl presented suffering from
asymmetrical linear streaks of hypo & hyper-pigmented atrophic lesions
with telangiectasia over her trunk and extremities, she had multiple
bone deformities especially of the limbs with facial asymmetry which
were confirmed by multiple X-rays. Abdominal examination was normal and
eye examination revealed myopia. Histopathological examination revealed
total dermal absence.
Introduction
Focal dermal hypoplasia (FDH) is a rare
meso-ectodermal disorder characterized by focal total dermal absence
with the epidermis directly overlying the subcutaneous tissue. It is
inherited by an X-linked dominant gene, which is lethal in homozygous
males. Occasional occurrence in males is due to fresh mutations. It was
first described by Goltz in 1962 [1].
Case Presentation
An 18 years old female presented to our outpatient
clinic at Al-Haud Al-Marsoud Hospital suffering from asymmetrical linear
streaks of hypo & hyper-pigmented atrophic lesions with telangiectasia
evident over her trunk (chest, abdomen, back & axillae) and extremities
(upper and lower limbs) (fig. 1-3).
 | Fig 1:
Asymmetrical linear streaks of hypo & hyper-pigmented atrophic
lesions with telangiectasia on face and extremities. |
|
 | Fig
2: Same lesions on lower extremities. |
|
 | Fig
3: Lesions on trunk (back and axillae).
|
|
On examination, she had multiple skeletal
anomalies in the form of multiple deformities of fingers and toes with
syndactyly of her left third and fourth toes. Asymmetry of all toes was
evident with nail dystrophy (fig. 4).
 | Fig
4: Multiple deformities of fingers and toes. |
|
Facial asymmetry was observed in the form of a
small rounded skull with triangular facial outline, asymmetry of the ala
nasi, pointed chin, prognathism, hypertrophy of the gums, irregular
teeth spacing and anomalous tooth form (fig.
5).
 | Fig
5: Small rounded skull, asymmetry of the ala nasi, pointed chin,
prognathism, hypertrophy of the gums, irregular teeth spacing and teeth
anomalies. |
|
General abdominal examination was done and
detected no abnormal findings and ocular examination diagnosed a myopic
eye.
Our clinical differential diagnoses included
Incontinentia pigmenti, MIDAS syndrome (microphthalmia, dermal aplasia,
and sclerocornea), lichen sclerosis et atrophicus and focal dermal
hypoplasia.
Investigations included multiple X-rays which
showed multiple bone deformities affecting both upper and lower limbs
including hands and feet (fig. 6).
 | Fig
6: Plain x-rays showing multiple bone deformities affecting
upper and lower extremities. |
|
Histopathological examination showed total absence
of the dermis so that the adipose tissue lies directly beneath the
epidermis (fig. 7).
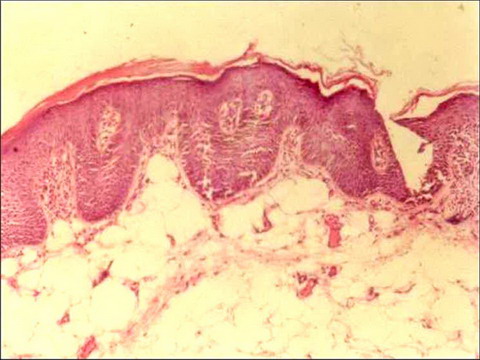 | Fig
7: H&E stained sections showing total absence of the dermis. |
|
Based on the previous findings, a diagnosis of
focal dermal hypoplasia (Goltz syndrome) was made.
Discussion
Focal dermal hypoplasia (Goltz Syndrome) is an
X-linked dominant mesoectodermal hypoplasia. It usually occurs in a
sporadic fashion and the affected persons are females, however it has
been reported occurring simultaneously with giant aplasia cutis
congenita in a newborn black male [2].
More than 200 cases have been reported, 90% of them are females who are
heterozygous or mosaic for mutations in PORCN; 10% are live-born
affected males who are mosaic for mutations in PORCN which has been
mapped to locus Xp11.23 [3].
It is usually bilateral but unilateral cases have been also described [4].
Our patient had most of the typical features of Goltz syndrome.
Goltz syndrome starts at birth and has a multitude
of clinical features including cutaneous, ocular, dental & skeletal
abnormalities. Skin involvement is essential for diagnosis in the form
of asymmetrical linear streaks of atrophy & telangiectasia which follows
Blaschko's lines. In racially pigmented skin, the lesions may be hypo or
hyper-pigmented. There is generalized dryness and pruritus with soft
reddish-yellow nodules (fat herniation). Raspberry-like papillomas occur
on the lips, perineum, ears, fingers, toes, buccal mucosa and
oesophagus. Nail absences or dystrophy with sparse & brittle hair are
evident. Characteristic facial features include the presence of a small
rounded skull, triangular facial outline, pointed chin, protruding ears
and asymmetrical ala nasi [5].
Our patient suffered from all the previous signs except for the skin
herniations and papillomas.
Oral and dental anomalies include prognathism,
agenesis, hypodontia, oligodontia, microdontia, enamel fragility and
dysplasia, retarded eruption, irregular teeth spacing, enamel defects
and malocclusion. Hypertrophy of the gums, high-arched palate; cleft
lip, palate, papillomas of the gums, tongue, palate & buccal mucosa may
all take place [6].
Warburg observed microphthalmia with bilateral coloboma of the iris and
ectopia lentis [7].
Other ocular lesions described are strabismus, anophthalmia, keratoconus
and corneal opacification [8].
Most of those findings were found to be consistent with our patient.
Skeletal anomalies include short stature with
asymmetric involvement of the hands and feet in 60% of patients,
including syndactyly, ectrodactyly, polydactyly, absence or hypoplasia
of digits and even absence of an extremity. Cervical rib has been
reported [9].
Scoliosis occurs in 20% of cases. Skeletal asymmetry, clavicular
dysplasia and spina bifida occulta can occur. The characteristic
radiological change is osteopathia striata of the long bones [10].
Our patient had multiple skeletal anomalies like osteopathia striata,
syndactyly and asymmetrical fingers and toes.
Goltz reviewed this disorder in 1992 [11].
Patients with areas of total absence of skin at birth have been
reported. Apocrine gland anomalies and hidrocystomas near the eyes also
have been described. Fibrovascular papillomas, especially in the
perianal and vulvar regions, are sometimes mistaken for condylomas.
Rarely, laryngeal and esophageal papillomas are seen. Osteopathia
striata is a frequent finding and 'lobster-claw' hand is a striking
feature of Goltz syndrome. Occasional anomalies include short stature,
joint hypermobility, mental retardation (15%), hearing defects,
microcephaly, horse-shoe kidneys, umbilical, inguinal, epigastric, or
diaphragmatic hernias [12].
Cardiac anomalies include cardiac tumors [13]
and congenital heart diseases like truncus arteriosus [14].
Other systems affection includes central nervous, gastrointestinal and
genitourinary systems affection [15].
Concerning management, skin lesions are not a
major therapeutic problem as the redness of early lesions tends to fade
with age, but facial lesions may be a cosmetic worry. Pruritus can be
troublesome and should not be overlooked. Constructive surgery and
vascular pulsed dye laser for telangiectatic skin lesions had been tried
[16].
Papillomata, particularly around the mouth, may be unsightly and can be
excised or ablated with cautery or cryotherapy; unfortunately they may
recur. Orthopaedic and plastic surgical advice should be sought early
with regard to limb deformities. Dental management is important and
education regarding caries is imperative. Although developmental delay
is more likely in more severely affected children, the degree cannot
accurately be predicted and is independent of any of the other features
of FDH. Regarding the prognosis, the majority of patients can lead a
normal life. Where reported, menses have occurred at a normal age [8].
References
1. Goltz RW, Peterson WC Jr, Gorlin RJ, Ravits HG: Focal
dermal hypoplasia. Arch Derm 1962; 86: 708- 717.
2. Gnamey DK, Koffi KS, Nagalo K, Guedenon KM, Akakpo-Numado
GK, Balaka B, Tatagan-Agbi K, Atakouma DY: Aplasia cutis congenita associated
with Goltz syndrome in a male neonate. Genet Couns. 2010; 21(1): 41- 47.
3. Naritomi K, Izumikawa Y, Nagataki S, Fukushima Y, Wakui
K, Niikawa N: Combined Goltz and Alicardi syndromes in a terminal XP deletion;
are they a contiguous gene syndrome? Am J Med Genet 1992; 43: 839- 843.
4. Aoyama M, Sawada H, Shintani Y, Isomura I, Morita A:
Case of unilateral focal dermal hypoplasia (Goltz syndrome). J Dermatol.
2008 Jan; 35(1): 33-35.
5. Quain RD, Militello G, Junkins-Hopkins J, Yan AC, Crawford
GH: Erythematous atrophic macules and papules following the lines of Blaschko.
Focal dermal hypoplasia (FDH), or Goltz syndrome. Arch Dermatol. 2007 Jan;
143(1): 109- 114.
6. Premalatha S, Augustine SM, Thambaiah AS: Focal dermal
hypoplasia syndrome - a case report. Indian Pediatr 1978; 15: 443- 444.
7. Warburg M: Focal dermal hypoplasia: ocular and general
manifestations with a survey of the literature. Acta Ophthal 1970; 48: 525-
536.
8. Temple IK, MacDowall P, Baraitser M, Atherton DJ: Focal
dermal hypoplasia (Goltz syndrome). J Med Genet 1990; 27: 180-187.
9. Ogunbiyi AO, Adewole IO, Ogunleye O, Ogunbiyi JO, Ogunseinde
OO, Baiyeroju-Agbeja A: Focal dermal hypoplasia: a case report and review
of literature. West Afr J Med 2003; 22: 346- 349.
10. Goltz RW, Henderson RR, Hitch JM, Ott JE: Focal dermal
hypoplasia syndrome. A review of the literature and report of two cases.
Arch Derm 1970; 101: 1-11.
11. Goltz RW: Focal dermal hypoplasia syndrome: An update.
Arch Derm 1992; 128: 1108- 1111.
12. Patel JS, Maher ER, Charles AK: Focal dermal hypoplasia
Goltz syndrome presenting as a severe fetal malformation syndrome. Clin
Dysmorphol 1997; 6: 267- 272.
13. Doede T, Seidel J, Riede FT, Vogt L, Mohr FW, Schier
F: Occult, life threatening, cardiac tumor in syndactylism in Gorlin-Goltz
syndrome. J Pediatr Surg 2004; 39: e17- 9.
14. Han XY, Wu SS, Conway DH, Pawel BR, Punnett HH, Martin
RA: Truncus arteriosus and other lethal internal anomalies in Goltz syndrome.
Am J Med Genet 2000; 90: 45- 48.
15. Reddy J, Laufer MR: Congenital anomalies of the female
reproductive tract in a patient with Goltz syndrome. J Pediatr Adolesc Gynecol.
2009 Aug; 22(4): e71- 2.
16. Sutton VR, Van den Veyver IB: Focal Dermal Hypoplasia.
In: Pagon RA, Bird TC, Dolan CR, Stephens K, editors. Gene Reviews [Internet].
Seattle (WA): University of Washington, Seattle; 2008 May 15.
© 2010 Egyptian Dermatology Online Journal
|
