|
|
|
Summary
A 60 years old female patient presented with
tender annular erythematous plaques, of two weeks duration, distributed
all over the body. Histopathological examination revealed flame figure
appearance of perivascular eosinophilic infiltrate.
Introduction
Wells' syndrome was first described by George
Wells as a recurrent granulomatous dermatitis with eosinophilia in 1971
[1].
Wells and Smith renamed it eosinophilic cellulitis in 1979 [2].
Wells' syndrome is rare; only about 80 cases have been reported
internationally. It usually affects adults, but it has been known to
occur in children as well with no race or sexual predilection [3,4].
The disease is often sporadic, but some familial cases have been
reported. There are suggested precipitating factors including: arthropod
bites, cutaneous viral infections, cutaneous parasitic infestations,
myeloproliferative disorders, atopic dermatitis and hypersensitivity
reactions to medications [5].
Wells' syndrome usually presents as a tender or
mildly pruritic cellulitis-like eruption, occasionally, papular and
nodular eruptions may be seen first [6].
The clinical picture can vary widely and may include: annular plaques,
urticaria and edema [7]
or vesicles and bullae. Bullous Wells' syndrome - are associated with
non-Hodgkin lymphoma [8].
Systemic symptoms such as: asthma, arthralgia and fever may occur.
Complete resolution of the disease with no scaring is the rule.
Case Presentation
A 60 years old female patient presented with
tender annular plaques over the face, trunk and extremities (fig.
1- 2). The lesions progressed over two
weeks to become large, indurated plaques of edema and erythema, with
violaceous edges and no collar. No other lesions of the skin or mucous
membrane were found on examination. Routine investigations were done
including: complete blood picture, liver function tests, kidney function
tests, erythrocyte sedimentation rate and blood sugar level. They were
all normal with the exception for mild elevation of leucocytic count and
eosinophilia in addition to elevated liver enzymes. Differential
diagnosis of this condition included: Wells' disease, granuloma annulare,
annular erythema and chronic eosinophilia.
 | Fig 1:
Annular erythematous plaques over the face and trunk. |
|
 | Fig
2: The annular erythematous plaques affecting the trunk and
extremities. |
|
Histopathological examination (fig.
3- 5) revealed superficial & deep
perivascular infiltrate which was rich in eosinophils giving flame
figures appearance. Diagnosis thus was well's syndrome.
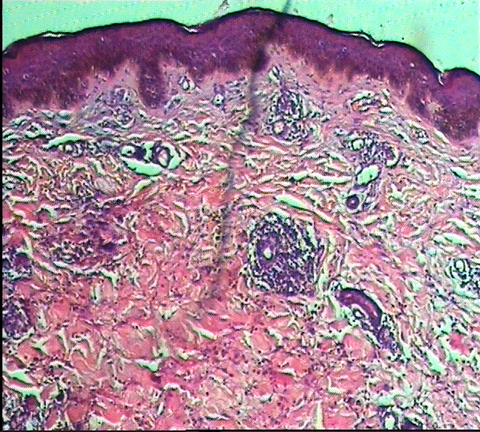 | Fig
3: H&E stained sections showing superficial & deep
perivascular infiltrate. |
|
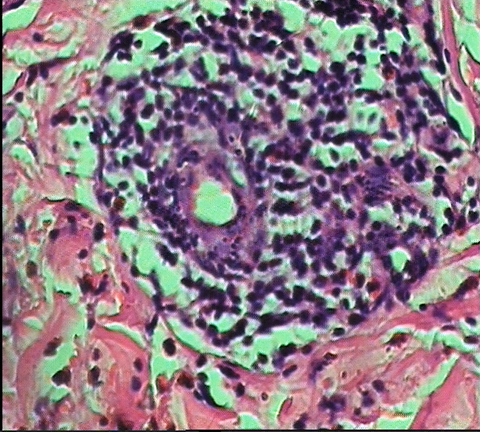 | Fig
4: The perivascular infiltrate was rich in eosinophils. |
|
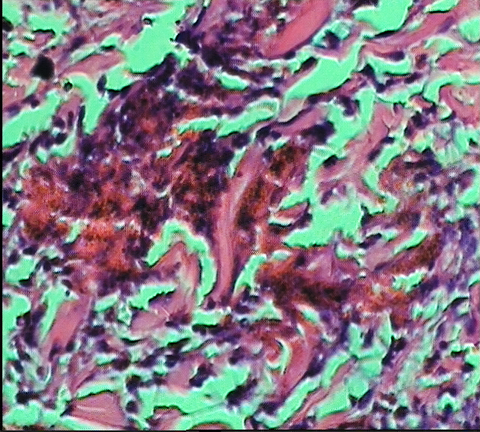 | Fig
5: The flame figures characteristic of the syndrome. |
|
Discussion
Eosinophilic cellulitis (Wells' syndrome) is an
uncommon condition of unknown etiology. An abnormal or dysregulated
eosinophil response appears to be implicated. The presentation usually
involves a mildly pruritic or tender cellulitis- like eruption but can
take the form of annular plaques as seen in our case with typical
histologic features characterized by edema, flame figures, and a marked
infiltrate of eosinophils in the dermis [9].
Some authors do not believe that Wells' syndrome
is a distinct clinical entity, but rather consider it a histopathologic
reaction pattern common to multiple disorders characterised by tissue
eosinophilia [10].
Others emphasize that the diagnosis should be reserved for cases with
typical features, characteristic histopathology and recurrent course.
Although the histopathologic findings of
eosinophilia, histiocytes, and flame figures are characteristic of
Wells' disease, they are also found in other conditions, including
bullous pemphigoid, eczema, tinea infection, and insect bites [11].
Complete resolution with no scarring is typical,
but scarring alopecia may occur in some cases. Although systemic
steroids appear to be the only therapeutic modality of benefit in Wells'
syndrome, anti-histaminics and dapsone have been found to be useful.
References
1. Wells GC. Recurrent granulomatous dermatitis with eosinophilia.
Trans St Johns Hosp Dermatol Soc. 1971; 57(1): 46- 56.
2. Wells GC, Smith NP. Eosinophilic cellulitis. Br J Dermatol.
Jan 1979; 100(1): 101- 109.
3. Anderson CR, Jenkins D, Tron V, Prendiville JS. Wells'
syndrome in childhood: case report and review of the literature. J Am Acad
Dermatol. Nov 1995; 33(5 Pt 2): 857- 864.
4. Nielsen T, Schmidt H, Sogaard H. Eosinophilic cellulitis.
(Well's syndrome) in a child. Arch Dermatol. Jul 1981; 117(7): 427- 429.
5. Odia SG, Purschel W, Worret WI, Rakoski J. Hypereosinophilic
cellulitis(Wells' syndrome) resembling urticaria. Acta Derm Venerol (Ljubljana).
1994; 6: 193- 195
6. Espana A, Sanz ML, Sola J, Gil P. Wells' syndrome (eosinophilic
cellulitis): correlation between clinical activity, eosinophil levels, eosinophil
cation protein and interleukin-5. Br J Dermatol. Jan 1999; 140(1): 127-
130.
7. Ghislain PD, Van Eeckhout P. Eosinophilic cellulitis
of papulonodular presentation (Wells' syndrome). J Eur Acad Dermatol Venereol.
Mar 2005; 19(2): 226- 227.
8. Spinelli M, Frigerio E, Cozzi A, Garutti C, Garavaglia
MC, Altomare G. Bullous Wells' syndrome associated with non-Hodgkin's lymphocytic
lymphoma. Acta Derm Venereol. 2008; 88(5): 530- 531.
9. Brehmer-Andersson E, Kaaman T, Skog E, Frithz A. The
histopathogenesis of the flame figure in Wells' syndrome based on five cases.
Acta Derm Venereol. 1986; 66(3): 213- 219.
10. Scharr WF, Tauscheck Al, Dickson KB, Melski JW. Eosinophilic
cellulitis (Wells' syndrome): histopathologic and clinical features in arthropod
bite reaction. J Am Acad Dermatol 1984; 11: 1043-1049.
11. Aberer W, Konrad K, Wolff K. Wells' syndrome is a distinctive
disease entity and not a histologic diagnosis. J Am Acad Dermatol. Jan 1988;
18(1 Pt 1):105-114.© 2010 Egyptian Dermatology
Online Journal
|
