|
|
Abstract
Lichen sclerosus et atrophicus (LSA) is a rare chronic inflammatory
dermatosis with anogenital and extragenital presentations. Extragenital
lichen sclerosus is most common on the neck, shoulders, and upper
portion of the trunk. Linear lesions are uncommon in LSA and very few
such cases are reported.
We describe a 5-year-old female child with unilateral linear
extra-genital lichen sclerosus. The lesions were confined to the left
lower extremity linearly along the left foot, left knee, thigh and a
lesion on the left side of her abdomen. Histological findings obtained
from the thigh lesion were those of typical LSA.
Introduction
Lichen sclerosus (LS) is a chronic dermatitis predominantly found in
the anogenital area. It can be found in patients of any age group, sex,
or race. Linear extragenital lichen sclerosus represents an
exceptionally rare form of lichen sclerosus. We report a case of
extra-genital linear lichen sclerosus et atrophicus in a child. This
case suggests that there is a linear form in LSA as already recognized
in localized scleroderma and it can occur in children also.
Case report
A 5-year-old female child was brought with asymptomatic linear skin
lesions involving her left leg and the left side of her abdomen that had
appeared, at the age of 4. Initially, his parents noted a group of
small, shiny white flat lesions located over the dorsum of the left
foot. Over the following few months, the similar lesions also appeared
over leg, near the knee, thigh and abdomen, coalesced into patches,
assuming the form of a linear lesion. Some of them were depressed,
wrinkled and slightly atrophic. There was no history of any genital
lesions or complaints. Parents denied history of any past treatment.
On examination, lesions consisted of sharply demarcated,
hypo-pigmented, atrophic, depressed, wrinkled, confluent, and isolated
patches in a linear configuration, along the left lower extremity and
left side of abdomen. (Fig1)
 | Fig 1:
Multiple hypopigmented patches over left lower extremity and
left side of abdomen running linearly. |
|
On the left abdominal wall, there was a parchment like patch.
(Fig 2) There was no underlying bony atrophy. Rest of her cutaneous
examination was normal including genital examination.
 | Fig
2: Close-up view of multiple atrophic, whitish patches over
left foot, knee and thigh and abdomen. |
|
A provisional diagnosis of linear lichen sclerosus, lichen striatus
or linear nevus depigmentosus was thought clinically.
Skin biopsy specimen taken from thigh lesion, showed features
consistent with lichen sclerosus et atrophicus including epidermal
atrophy, vacuolar alteration of dermo-epidermal junction, hyalinized
papillary dermal collagen and few melanophages with sparse superficial
perivascular lymphocytic infiltrate. (Fig 3, 4)
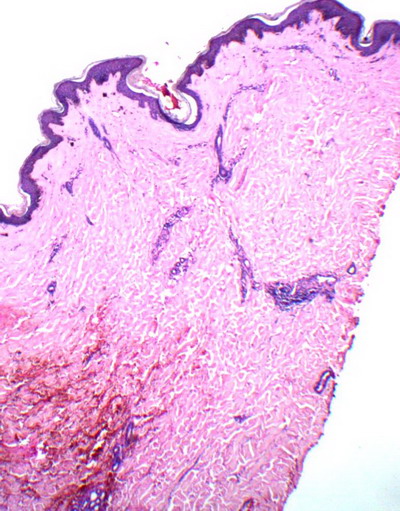 | Fig
3: Skin biopsy from thigh lesion showing atrophic epidermis,
vacuolar interface and hylinized papillary dermis. (H&E, 40X) |
|
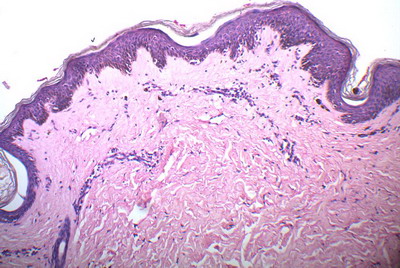 | Fig
4: High power view showing hylinized collagen, lymphocytic
infiltrate, melanophages and slightly atrophic epidermis with
interface. (H&E, 100X) |
|
Hemogram, autoantibody screen, liver, kidney, and thyroid function
tests were normal. Borrelia burgdorferi serology was not done due to
cost constraints of patient.
Based on clinico-pathological correlation a diagnosis of linear
extragenital lichen sclerosus was made. Patient was advised clobetasol
propionate 0.05% cream along with moisturizers and is under follow-up.
Discussion
Lichen sclerosus (LS) is a chronic dermatitis affecting
predominantly, the anogenital area. It can be found in patients of any
age group, sex, or race, but is most commonly present in peri- or
postmenopausal women. Although the etiology of LS remains uncertain, an
autoimmune process is believed to underlie this condition. [1]
Extragenital lichen sclerosus without accompanying genital lesions
was recorded in 805 of 4280 cases reviewed by Meffert et al.[2]
Extragenital lichen sclerosus is most common on the neck, shoulders, and
upper portion of the trunk. It is generally asymptomatic, but
occasionally pruritic. Most lesions of extragenital lichen sclerosus
present as flat, white, polygonal papules, and slight atrophic white
plaques. [3]
Extragenital lichen sclerosus with linear lesions or following the
lines of Blaschko represents rare presentation of lichen sclerosus.
In 1995, Izumi et al. [4] were the
first to describe a linear form of lichen sclerosus extending from the
left upper back and along the left arm, probably following the lines of
Blaschko. Okamoto et al added another case of linear lichen sclerosus in
a 23-year-old woman who developed initial lesions at the age of 18. [2,4]
Location of lesions preferentially on left side of body in most of
the reported cases has been attributed to stronger cell-mediated immune
hypersensitivity in the left side of the body than the right in healthy
young subjects and it is speculated that the cellular immune
responsiveness might influence the confinement of the Blaschko-linear
lichen sclerosus to the left side of the body. [3,5]
In our case also, lesions were located on left lower extremity and left
side of abdomen and probably were following lines of Blaschko supporting
above speculation. The lines of Blaschko were described and drawn in
1901 by Alfred Blaschko (1858-1922), a private practitioner of
dermatology in Berlin. In disorders that affect skin areas corresponding
to Blaschko's lines, it is believed that two distinct cell clones arise
early in embryogenesis, often produced by genetic mosaicism.[2,6]
Various acquired conditions that can follow Blaschko's lines include
lichen striatus, linear psoriasis, linear lichen planus, linear
scleroderma, linear atrophoderma etc. [6]
Our case thus presents a rare presentation of lichen sclerosus with
linear and unilateral extragenital lesions in a child.
References
1. Funaro, D. Lichen sclerosus: a review and practical
approach. Dermatologic Therapy, 2004;17: 28-37
2. Choi SW, Yang JE, Park HJ, Kim CW. A case of
extragenital lichen sclerosus following Blaschko's lines. J Am Acad
Dermatol 2000;43:903-4
3. Pavlovic MD. Linear lichen sclerosus with underlying
bony atrophy. J Am Acad Dermatolo 2004;50(3):E4
4. Izumi T, Tajima S. A case of linear type of lichen
sclerosus et atrophicus? J Dermatol 1995; 22: 279- 82.
5. Dane S, Erdem T, Gumustekin K. Cell-mediated immune
hypersensitivity is stronger in the left side of the body than the right
in healthy young subjects. Percept Mot Skills 2001; 93: 329- 32.
6. Tagra S, Talwar AK, Walia RS. Lines of Blaschko.
Indian J Dermatol Venereol Leprol 2005; 71: 57- 9
© 2011 Egyptian Dermatology Online Journal
|
